

Association of C reactive protein triglyceride glucose index with mortality in coronary heart disease and type 2 diabetes from NHANES data
- PMID: 40634472
- PMCID: PMC12241523
- DOI: 10.1038/s41598-025-10184-x
Association of C reactive protein triglyceride glucose index with mortality in coronary heart disease and type 2 diabetes from NHANES data
Abstract
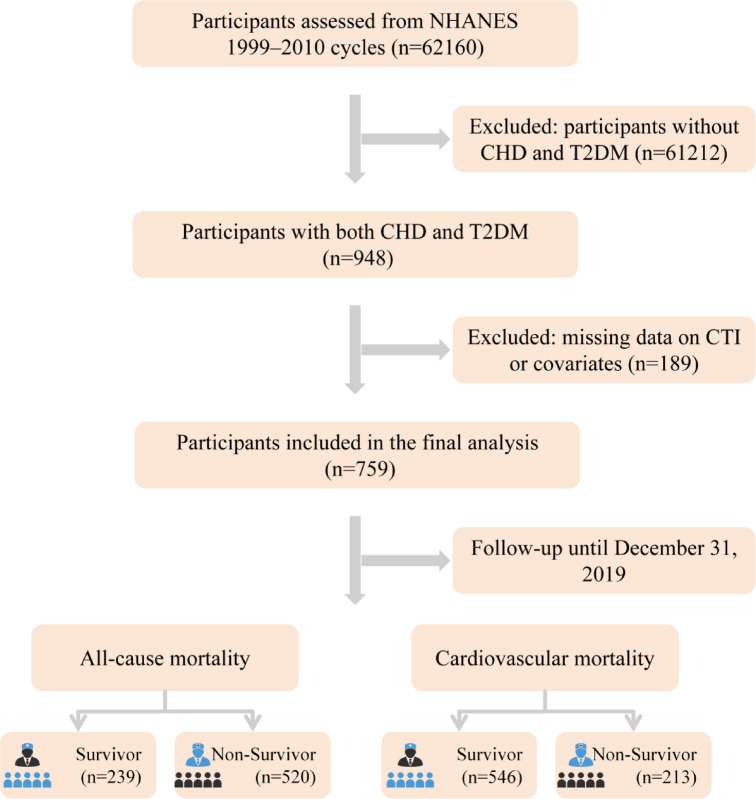
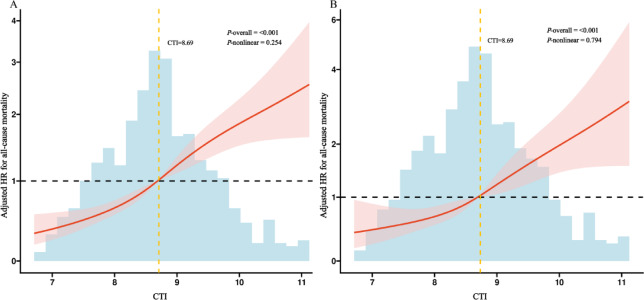
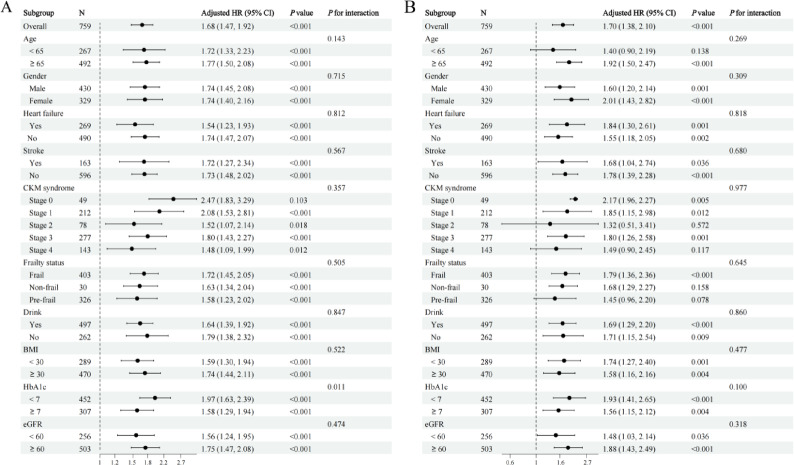
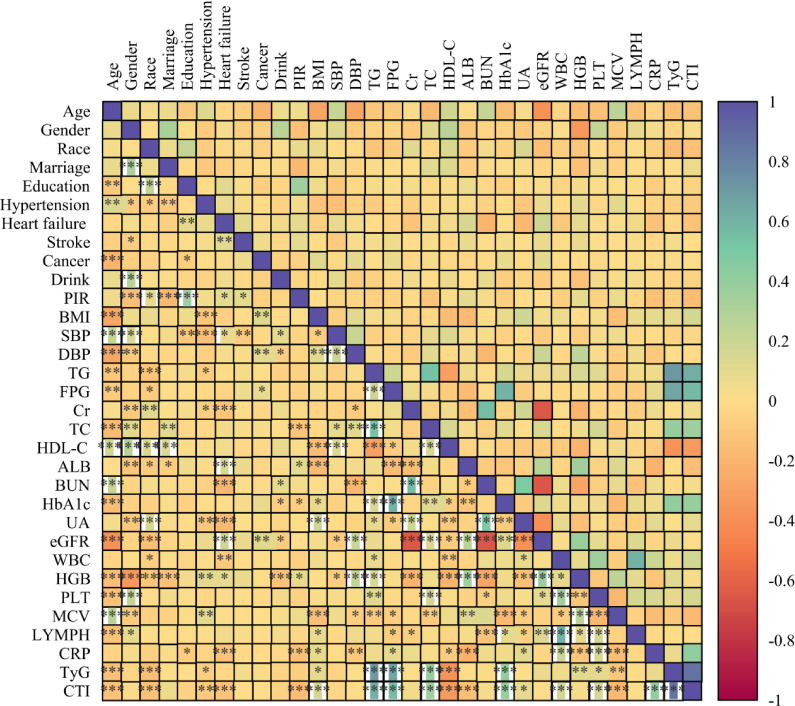
Coronary heart disease (CHD) and type 2 diabetes mellitus (T2DM) frequently coexist, significantly elevating the risk of adverse cardiovascular outcomes and mortality. The C-reactive protein-triglyceride-glucose index (CTI), a novel composite marker reflecting both inflammation and insulin resistance, has been associated with poor prognosis in various populations. However, its relationship with all-cause and cardiovascular mortality in patients with coexisting CHD and T2DM remains unclear. Data were obtained from 759 adults with both CHD and T2DM enrolled in the National Health and Nutrition Examination Survey (NHANES) 1999-2010 cycles, with mortality follow-up through December 31, 2019. CTI was calculated and categorized into quartiles. Kaplan-Meier survival analysis, multivariable Cox proportional hazards models, and restricted cubic spline (RCS) analyses were performed to assess the association between CTI levels and risks of all-cause and cardiovascular mortality. Pearson correlation analyses were conducted to evaluate the associations between CTI and key metabolic and inflammatory markers. Subgroup analyses were performed to assess the robustness and consistency of the associations across different clinical strata. During a median follow-up of 109 months, 520 all-cause deaths and 213 cardiovascular deaths were recorded. Higher CTI levels were independently associated with increased risks of both all-cause (HR: 1.68; 95%CI: 1.47-1.92) and cardiovascular mortality (HR: 1.70; 95%CI: 1.38-2.10) after full adjustment (P for trend < 0.001). RCS analysis confirmed a linear dose-response relationship. The association was consistent across subgroups, with stronger effects observed in patients with HbA1c < 7%. CTI also showed significant correlations with multiple metabolic and inflammatory markers.nteraction analyses further revealed that the association between CTI and all-cause mortality was more pronounced in younger individuals (P for interaction = 0.012), while no significant effect modification was observed across cardiovascular-kidney-metabolic stages or frailty status. Findings remained robust in survey-weighted analyses, and CTI also showed strong correlations with a range of metabolic and inflammatory biomarkers, supporting its integrative prognostic utility. Elevated CTI is independently associated with higher all-cause and cardiovascular mortality risks in patients with CHD and T2DM. CTI may serve as a valuable biomarker for risk stratification in this high-risk population. Further studies are warranted to validate its clinical utility.
Keywords: All-cause mortality; C-reactive protein-triglyceride-glucose index; Cardiovascular mortality; Coronary heart disease; NHANES; Type 2 diabetes mellitus.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: NHANES was conducted with approval by the National Center for Health Statistics Ethics Review Board, and obtained informed written consent from all the individuals involved in the study. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests. Author details. 1Department of Cardiology, The Second Affiliated Hospital of Xuzhou Medical University, Xuzhou, 221000, China.
Figures


References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
