

A Case Report of Acute on Chronic Osteomyelitis of Distal Femur Managed with Sequestrectomy, Saucerization, and Stimulan Placement
- PMID: 40635932
- PMCID: PMC12237473
- DOI: 10.13107/jocr.2025.v15.i07.5808
A Case Report of Acute on Chronic Osteomyelitis of Distal Femur Managed with Sequestrectomy, Saucerization, and Stimulan Placement
Abstract
Introduction: Osteomyelitis is a bone infection that may present acutely or chronically. Acute on chronic osteomyelitis refers to the exacerbation of symptoms in a patient with an underlying chronic infection. This case report presents a 19-year-old male diagnosed with acute on chronic osteomyelitis of the right distal femur, with no history of a discharging sinus for the past 6 months. Osteomyelitis is a bone infection commonly caused by bacteria, with Staphylococcus aureus being the most frequent pathogen. Chronic osteomyelitis can occasionally experience acute flare-ups, referred to as "acute on chronic osteomyelitis". This report discusses the presentation, diagnosis, and management of a 19-year-old male with acute on chronic osteomyelitis of the right distal femur.
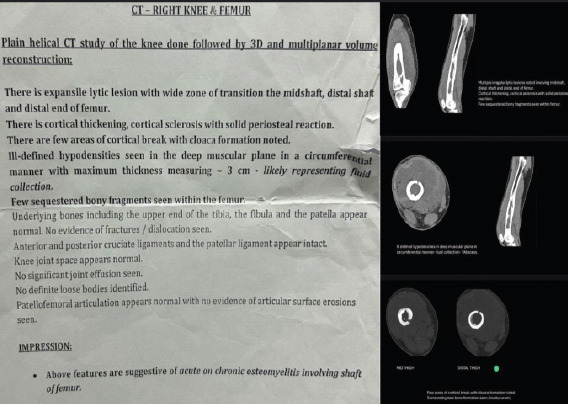
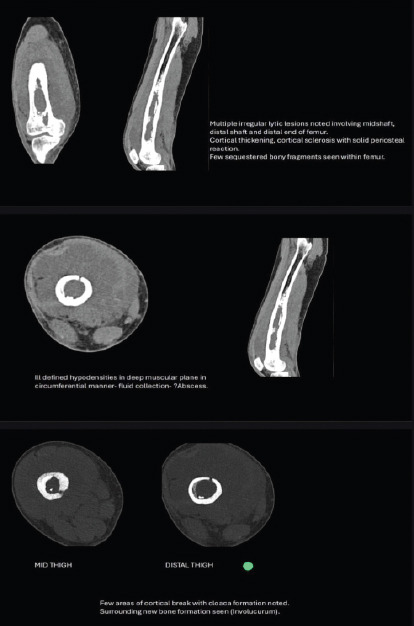
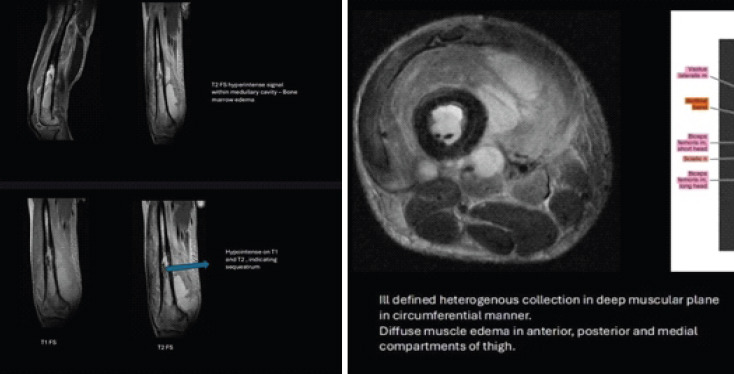
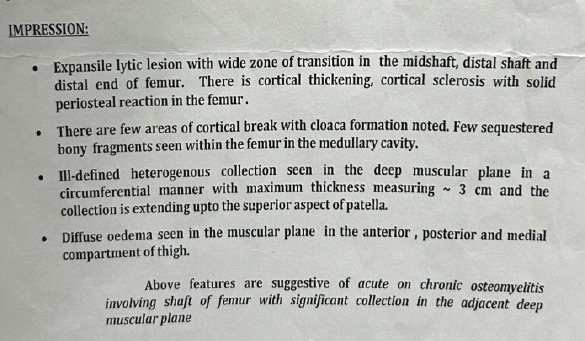
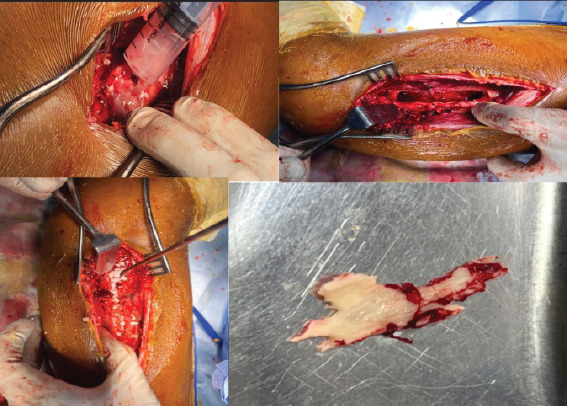
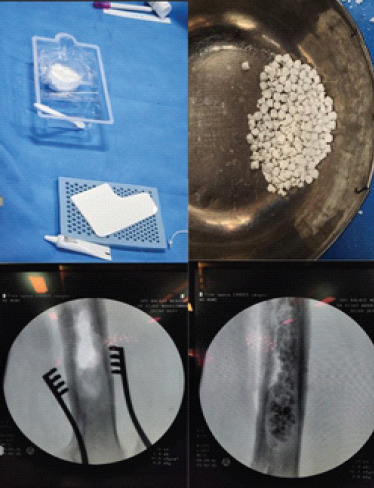
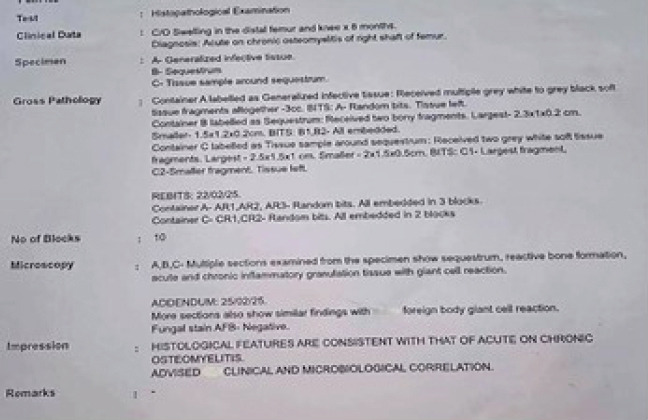
Case report: A 19-year-old male presented with increasing pain, swelling, and warmth over his right distal femur for 2 weeks. The pain was deep, throbbing, worsened by weight-bearing, and unrelieved by analgesics. He had similar complaints 6 months ago but had no symptoms such as fever or discharging sinus since then. There was no history of trauma or injury. On physical examination, the patient exhibited localized tenderness, mild swelling, broadening, irregularity, and warmth over the distal femur. Movements of the knee were restricted, and pain was elicited with direct palpation of the femur. No open wounds or discharging sinuses were present, and neurological and vascular examinations were unremarkable.Radiographs of the right femur showed sclerosis and focal cortical thickening, indicating chronic osteomyelitis. Magnetic resonance imaging confirmed the presence of marrow edema, cortical irregularity, and periosteal reaction, supporting the diagnosis of chronic osteomyelitis with an acute exacerbation. Blood tests revealed an elevated white blood cell count and C-reactive protein, indicating an acute inflammatory response. The patient received intravenous antibiotics preoperatively, followed by sequestrectomy, saucerization, and stimulan placement over the site where necrotic bone was removed to promote healing. Over 6 weeks, the patient experienced significant improvement in symptoms. Repeat imaging showed resolution of the acute infection, and long-term oral antibiotics were prescribed to manage chronic osteomyelitis.This case emphasizes the challenges of diagnosing and treating acute on chronic osteomyelitis, particularly when typical signs like a discharging sinus are absent. Early diagnosis and prompt, targeted antibiotic therapy is crucial for preventing complications such as deformities, limb loss, or sepsis.
Conclusion: Effective management of acute on chronic osteomyelitis requires comprehensive evaluation through clinical history, imaging, and laboratory testing. Early intervention with surgical debridement and appropriate antibiotic therapy is vital to achieving favorable outcomes and preventing long-term complications.
Keywords: Acute on chronic osteomyelitis; distal femur; stimulan.
Copyright: © Indian Orthopaedic Research Group.
Conflict of interest statement
Conflict of Interest: Nil
Figures



Similar articles
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Can we improve time to patency with vasoepididymostomy with an innovative epididymal occlusion stitch?Int Braz J Urol. 2024 Jul-Aug;50(4):504-506. doi: 10.1590/S1677-5538.IBJU.2024.0222. Int Braz J Urol. 2024. PMID: 38743068 Free PMC article.
-
Sexual Harassment and Prevention Training.2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 36508513 Free Books & Documents.
-
Does Augmenting Irradiated Autografts With Free Vascularized Fibula Graft in Patients With Bone Loss From a Malignant Tumor Achieve Union, Function, and Complication Rate Comparably to Patients Without Bone Loss and Augmentation When Reconstructing Intercalary Resections in the Lower Extremity?Clin Orthop Relat Res. 2025 Jun 26. doi: 10.1097/CORR.0000000000003599. Online ahead of print. Clin Orthop Relat Res. 2025. PMID: 40569278
References
-
- Lew DP, Waldvogel FA. Osteomyelitis. Lancet. 2004;364:369–79. - PubMed
-
- Calhoun JH, Manring MM. Adult osteomyelitis. Infect Dis Clin North Am. 2005;19:765–86. - PubMed
-
- Saeed K, McLaren AC, Schwarz EM. Diagnosing and managing chronic infection in orthopaedics:Practical implications of evolving techniques and technologies. J Bone Joint Surg Am. 2021;103:e57.
-
- Llauger J, Palmer J, Amores S, Bagué S, Camins A. Osteomyelitis of the long bones:Radiologic diagnosis. Eur Radiol. 1998;8:1742–9.
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous