

Health outcomes up to 3 years and post-exertional malaise in patients after hospitalization for COVID-19: a multicentre prospective cohort study (CO-FLOW)
- PMID: 40636057
- PMCID: PMC12237789
- DOI: 10.1016/j.lanepe.2025.101290
Health outcomes up to 3 years and post-exertional malaise in patients after hospitalization for COVID-19: a multicentre prospective cohort study (CO-FLOW)
Abstract
Background: Many patients experience long-lasting health problems after COVID-19. The study aimed to assess 3-year trajectories of a comprehensive set of patient-reported outcome measures (PROMs) in patients hospitalized for COVID-19, particularly focusing on the 2- to 3-year trajectory. Additionally, we evaluated prevalence of post-exertional malaise (PEM) at 3 years, its risk factors, co-occurring health problems, and the 3-year trajectories of patients with and without PEM.
Methods: The CO-FLOW multicentre prospective cohort study followed up adults hospitalized for COVID-19 in 7 hospitals, located in the Netherlands. Study assessments were performed at 3, 6, 12, 24, and 36 months post-discharge, conducted between July 1, 2020, and May 22, 2024. PROMs on recovery, symptoms, fatigue, mental health, cognition, participation, sleep quality, work status, health-related quality of life (HRQoL), and PEM were collected. Generalized estimating equations were used to assess health trajectories and multivariable logistic regression to identify risk factors for PEM.
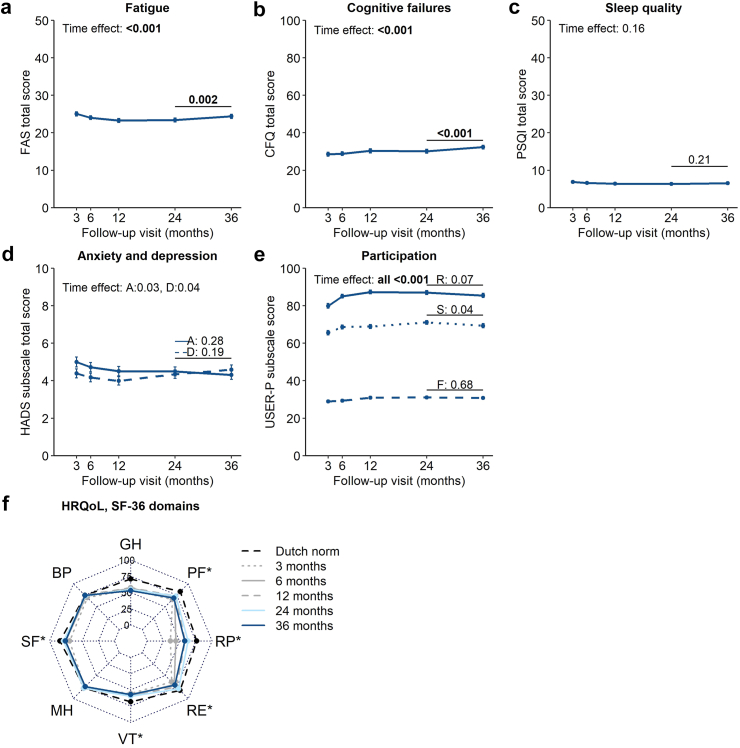
Findings: In total, 299/344 (87%) patients completed the 3-year follow-up and were included in the analysis. Complete recovery rates increased (p < 0.001), from 12% at 3 months to 24% at 3 years. Symptoms of impaired fitness, fatigue, and muscle weakness (all p < 0.0019) and PROMs for fatigue score, participation, return to work, and HRQoL (all p < 0.005) improved significantly over time, while PROMs for cognitive failures worsened (p < 0.001). Between the 2- and 3-year visits, memory problems (OR 1.4 [1.1-1.7], p < 0.001), and scores of fatigue (MD +1.0 [0.4-1.6], p = 0.002), cognitive failures (MD +2.2 [0.9-3.4], p < 0.001), and SF-36 mental component summary (-2.2 [-3.1 to -1.3], p < 0.001) significantly worsened. At 3 years, 66% of patients experienced fatigue, 63% impaired fitness, 59% memory problems, and 53% concentration problems. PROMs showed that 62% reported poor sleep quality, 55% fatigue, and 28% cognitive failures. PEM was reported by 105/292 (36%) patients at 3 years; risk factors were female sex (OR 3.4 [95% CI 1.9-6.0], p < 0.001), pre-existing pulmonary disease (3.0 [1.7-5.6], p < 0.001), physical inactivity pre-COVID-19 (2.3 [1.2-4.1], p = 0.008), and ICU treatment for COVID-19 (1.8 [1.02-3.0], p = 0.04). Concurrent fatigue, cognitive failures, and dyspnea were more common in patients with (42%) than without (6%) PEM. Patients with PEM showed poor health outcomes throughout the entire follow-up period, including worsening fatigue and HRQoL during the third year.
Interpretation: Many health problems persisted up to 3 years post-discharge, with self-reported fatigue and cognitive problems worsening in the third year. PEM was common, and linked to a more severe phenotype of long COVID. These findings highlight the urgent need to optimize treatment options and investigate underlying pathological mechanisms of COVID-19.
Funding: The Netherlands Organisation for Health Research and Development (ZonMw); Rijndam Rehabilitation; Laurens.
Keywords: COVID-19; Long COVID; Long-term health outcomes; Post-exertional malaise.
© 2025 The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests related to this paper.
Figures



References
-
- World Health Organisation WHO coronavirus (COVID-19) dashboard. https://covid19.who.int/
-
- National Academies of Sciences, Engineering, and Medicine . 2024. A long COVID definition: a chronic, systemic disease state with profound consequences. - PubMed
-
- World Health Organisation . 2021. A clinical case definition of post COVID-19 condition by a Delphi consensus, 6 October 2021.
LinkOut - more resources
Full Text Sources
Research Materials
