

An investigation of the relationship between sPD-1, sPD-L1 and severe pneumonia patients admitted to ICU and its clinical significance
- PMID: 40636377
- PMCID: PMC12237637
- DOI: 10.3389/fmed.2025.1605653
An investigation of the relationship between sPD-1, sPD-L1 and severe pneumonia patients admitted to ICU and its clinical significance
Abstract
Background: Soluble programmed cell death 1 (sPD-1) and its ligand (sPD-L1) have emerged as potential biomarkers for early identification and risk stratification in patients with severe pneumonia (SP). However, there is a lack of robust laboratory evidence supporting their clinical utility. This study aimed to explore the relationship between sPD-1/sPD-L1 levels and clinical outcomes in SP patients.
Methods: This study included SP patients admitted to the Department of Critical Care Medicine at the Affiliated Hospital of Zunyi Medical University between November 2022 and December 2023. Patients were categorized into survivor and non-survivor groups based on 28-day clinical outcomes. Baseline characteristics and laboratory data were collected upon admission. Serum levels of sPD-1 and sPD-L1 were quantified using enzyme-linked immunosorbent assay. Cox regression analysis was performed to identify prognostic factors, and a nomogram was developed to predict outcomes. The predictive performance of sPD-1, sPD-L1, and their combined indices was evaluated using receiver operating characteristic (ROC) curve analysis.
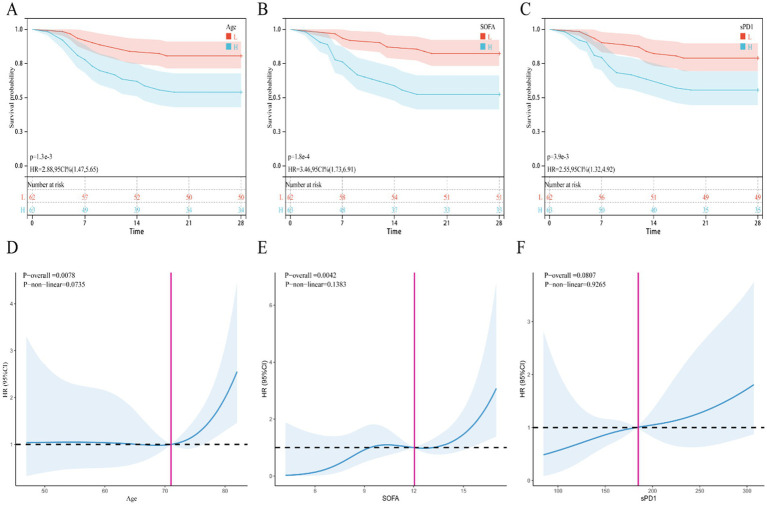
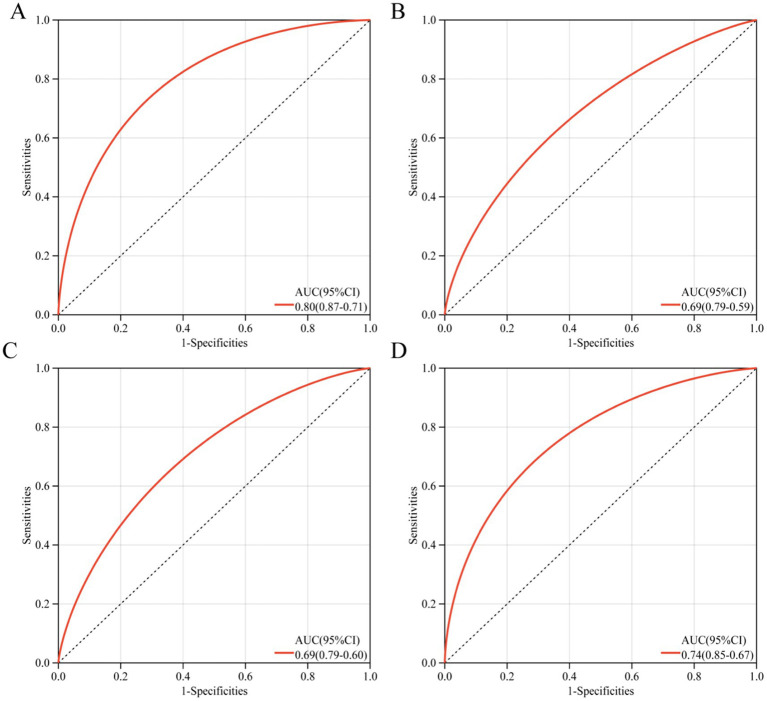
Results: A total of 125 patients with severe pneumonia (SP) were included in this study. Compared to survivors, non-survivors were older, had more severe disease (as indicated by higher SOFA and APACHE II scores), and exhibited lower body mass index (BMI), hemoglobin levels, lymphocyte counts, CALLY index, and albumin levels. Additionally, non-survivors showed significantly elevated levels of systemic inflammatory markers (NLR, PLR, MLR, CLR, CAR, and SII) and higher serum sPD-1 concentrations. Multivariate Cox regression analysis identified age, SOFA score, and sPD-1 levels as independent risk factors for poor prognosis in SP patients. Restricted cubic spline (RCS) curves revealed a linear relationship between age, SOFA score, and the risk of poor prognosis. A nomogram incorporating age, SOFA score, and sPD-1 levels demonstrated strong predictive performance for 28-day mortality in SP patients, with an area under the curve (AUC) of 0.80. Incorporating sPD-1 measurements significantly improves the prognostic accuracy of both SOFA and APACHE II scores in critically ill patients.
Conclusion: sPD-1 levels were significantly elevated in non-surviving SP patients, suggesting its potential role as a biomarker for disease severity and immune dysregulation. The combination of sPD-1 with other clinical parameters may provide valuable insights into the prognosis and immune status of SP patients.
Keywords: 28 day mortality rate; SPDL1; prognosis; severe pneumonia; soluble PD1.
Copyright © 2025 Gao, Lu, Yu and Fu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Systemic Inflammatory Response Syndrome.2025 Jun 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jun 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 31613449 Free Books & Documents.
-
[Clinical study on the effect of glycosaminoglycans on vascular endothelial glycocalyx in sepsis].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2025 Jun;37(6):527-534. doi: 10.3760/cma.j.cn121430-20240725-00634. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2025. PMID: 40820527 Chinese.
-
Machine learning-based model for predicting all-cause mortality in severe pneumonia.BMJ Open Respir Res. 2025 Mar 22;12(1):e001983. doi: 10.1136/bmjresp-2023-001983. BMJ Open Respir Res. 2025. PMID: 40122535 Free PMC article.
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.Health Technol Assess. 2006 Sep;10(34):iii-iv, ix-xi, 1-204. doi: 10.3310/hta10340. Health Technol Assess. 2006. PMID: 16959170
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
References
LinkOut - more resources
Full Text Sources