

Anterior Interosseous Nerve to Pronator Quadratus Transfer to Restore Intrinsic Function: An Adjunct to Cubital Tunnel Decompression
- PMID: 40636629
- PMCID: PMC12240554
- DOI: 10.7759/cureus.85597
Anterior Interosseous Nerve to Pronator Quadratus Transfer to Restore Intrinsic Function: An Adjunct to Cubital Tunnel Decompression
Abstract
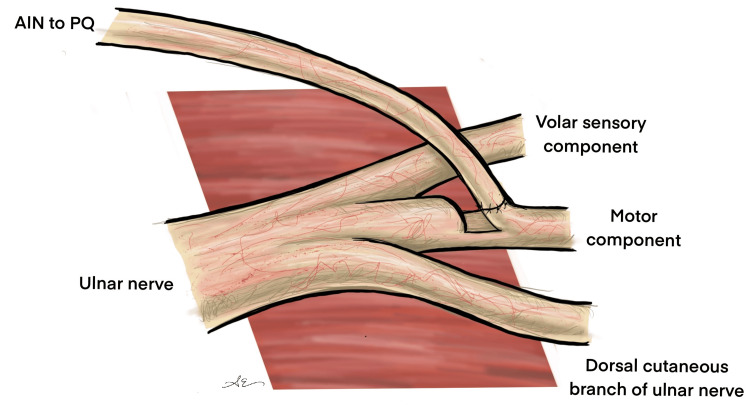
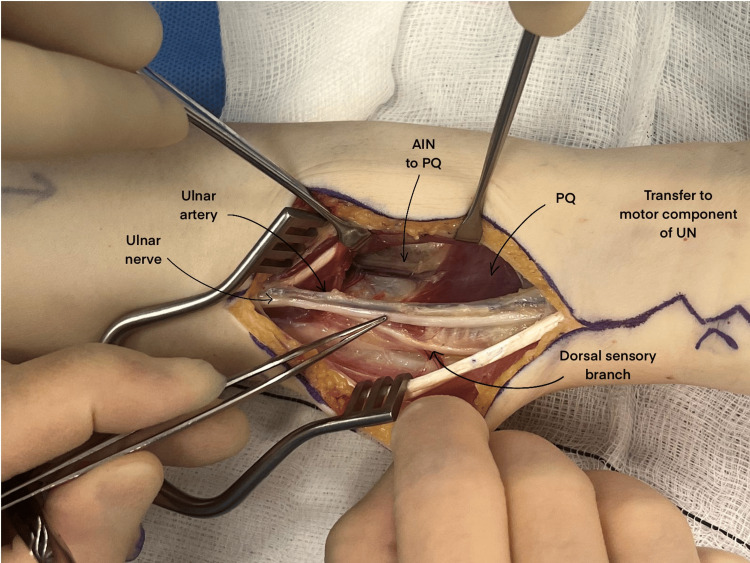
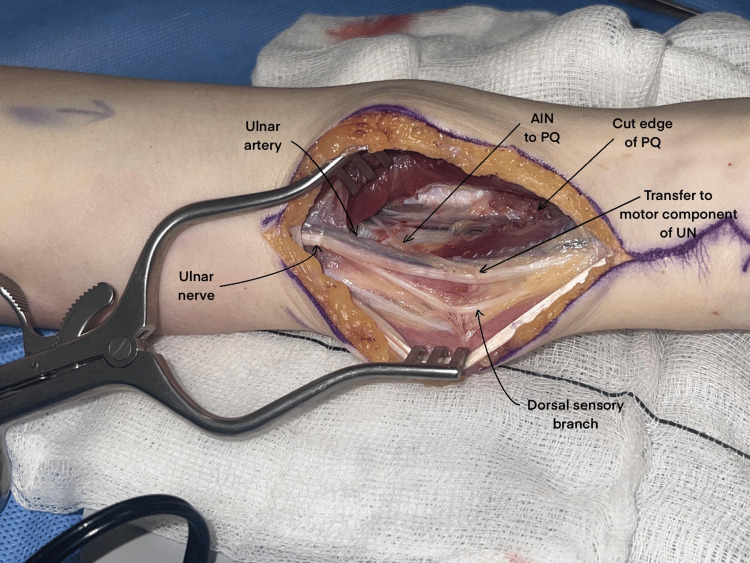
Background Injury or compression of the ulnar nerve impairs fine motor control, intrinsic hand function, and sensation in the small and ulnar side of the ring finger. Anterior interosseous nerve to pronator quadratus (AINPQ) transfer offers a potential solution, leveraging this expendable nerve to enhance the recovery of the ulnar nerve's motor function. Method This single-unit retrospective case series evaluates seven patients undergoing combined cubital tunnel decompression and AINPQ transfer for severe ulnar neuropathy. Data were collected from December 2020 to January 2023, including age, hand dominance, affected limb, and symptom duration (pain, sensory changes, motor weakness). The cohort comprised cases of both compressive and traumatic ulnar nerve injuries. Electrophysiological findings, intraoperative observations, postoperative assessments, and complications were recorded. Outcomes were measured using the Disabilities of the Arm, Shoulder, and Hand questionnaire at least six months postoperatively, with success defined as a ≥1 Medical Research Council (MRC) grade improvement or a score of >3 in thumb adduction, intrinsic function, or grip strength. Results All patients demonstrated a motor function improvement of ≥1 MRC grade following AINPQ transfer. The complication rate was low, with no reported cases of functional deterioration or infection, consistent with existing literature. One patient reported a painful scar, attributed to the cubital tunnel decompression procedure. Conclusion This study supports the adjunctive use of AINPQ with cubital tunnel decompression in severe ulnar nerve compression or injury cases. AINPQ shows potential in accelerating reinnervation and improving hand function within 12-14 months of symptom onset, though larger prospective studies are necessary for validating and refining patient selection criteria.
Keywords: ain; hemi-end-to-end; nerve; transfer; ulnar.
Copyright © 2025, Elfaki et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Supercharge end-to-side anterior interosseous-to-ulnar motor nerve transfer restores intrinsic function in cubital tunnel syndrome. Dengler J, Dolen U, Patterson JM, Davidge KM, Kahn LC, Yee A, Mackinnon SE. Plast Reconstr Surg. 2020;146:808–818. - PubMed
-
- Nerve transfer of the anterior interosseous nerve to the thenar branch of the median nerve - an anatomical and histological analysis. Frank K, Englbrecht M, Koban KC, Cotofana SC, Stewart JK, Giunta RE, Schenck TL. J Plast Reconstr Aesthet Surg. 2019;72:751–758. - PubMed
-
- A comparison of tendon and nerve transfer surgery for reconstruction of upper limb paralysis. Cavallaro D, Mikalef P, Power D. J Musculoskelet Surg Res. 2019;3:69.
-
- Evaluation and management of peripheral nerve injury. Campbell WW. Clin Neurophysiol. 2008;119:1951–1965. - PubMed
LinkOut - more resources
Full Text Sources