

Recent advances in alcohol metabolism: from the gut to the brain
- PMID: 40637545
- PMCID: PMC12345593
- DOI: 10.1152/physrev.00053.2024
Recent advances in alcohol metabolism: from the gut to the brain
Abstract
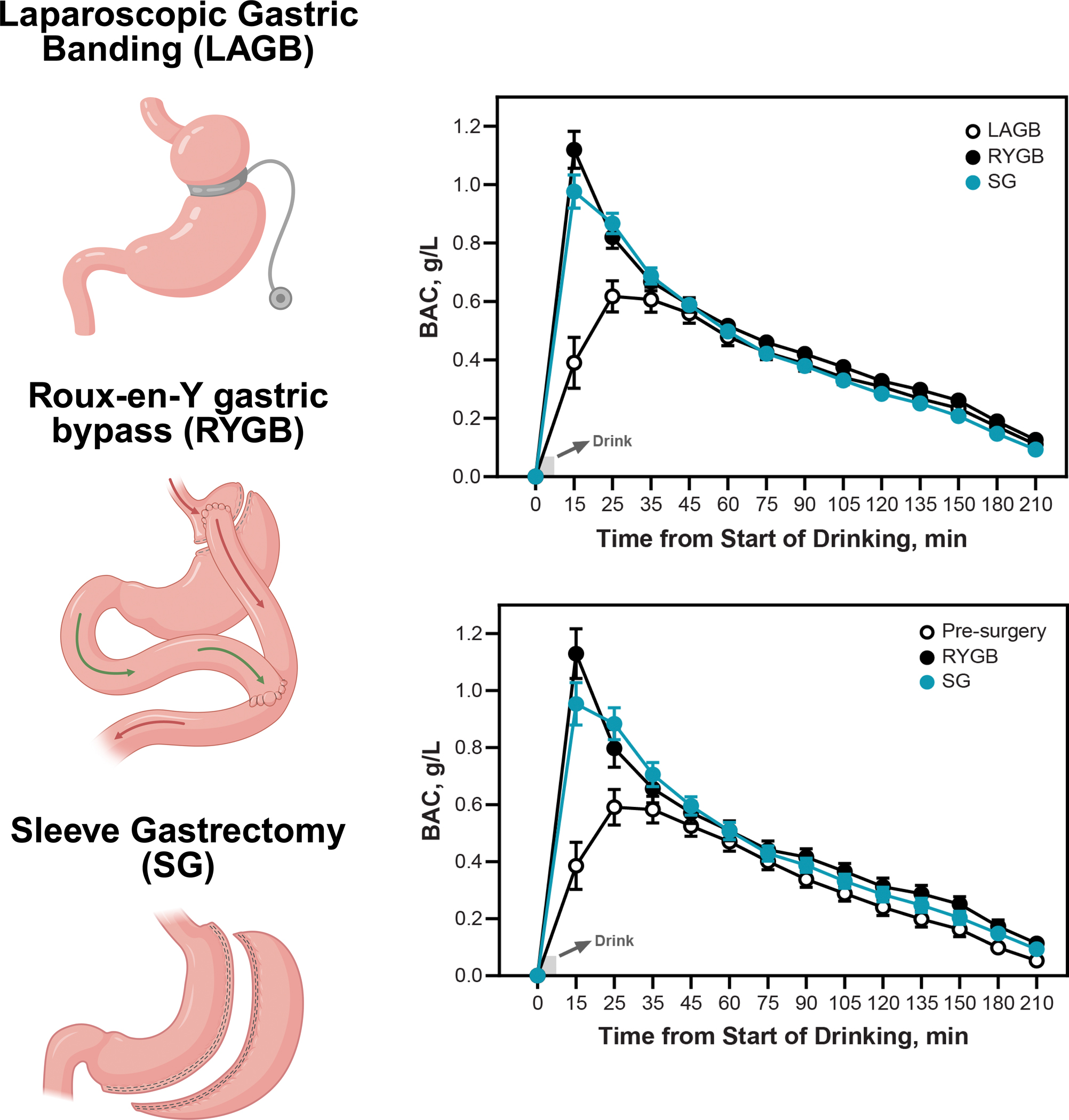
Globally, alcohol is the most widely used psychoactive drug and a leading cause of premature death among individuals aged 15-49 years. Understanding the absorption, distribution, metabolism, and excretion of alcohol in the human body, otherwise known as alcohol pharmacokinetics, is essential for predicting its behavioral effects and toxic consequences. This review examines the evolutionary origins of alcohol consumption and metabolism, focusing on the activity of alcohol dehydrogenase enzymes across species, which serve as key catalysts in alcohol oxidation. It also highlights recent advances in understanding central alcohol metabolism and updates on the potential clinical significance of nonoxidative pathways of alcohol metabolism and endogenous alcohol production, particularly in the context of liver disease. In addition, the review inspects factors that modulate alcohol metabolism, including genetic polymorphisms, biological sex, food intake, women's reproductive status, and clinical interventions such as medications and metabolic surgeries. Understanding these sources of variability in alcohol metabolism is crucial for identifying individual risk factors and tailoring strategies to reduce alcohol-related harm. This comprehensive review offers a current perspective on alcohol pharmacokinetics, valuable insights into its implications for health, behavior, and potential innovative therapeutic targets.
Keywords: acetaldehyde dehydrogenase; alcohol dehydrogenase; bariatric surgery; genetic polymorphisms; lactation.
Conflict of interest statement
Figures





References
-
- Griswold MG, Fullman N, Hawley C, Arian N, Zimsen SRM, Tymeson HD, Venkateswaran V, Tapp AD, Forouzanfar MH, Salama JS, et al. Alcohol use and burden for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. The Lancet 392, 2018. doi: 10.1016/S0140-6736(18)31310-2. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- Z01 AA000466/ImNIH/Intramural NIH HHS/United States
- Z1AAA000466/HHS | NIH | National Institute on Alcohol Abuse and Alcoholism (NIAAA)
- AA007611/HHS | NIH | National Institute on Alcohol Abuse and Alcoholism (NIAAA)
- AA024103/HHS | NIH | National Institute on Alcohol Abuse and Alcoholism (NIAAA)
- P50 AA007611/AA/NIAAA NIH HHS/United States
- AA008401T/HHS | NIH | National Institute on Drug Abuse (NIDA)
- DC011287/HHS | NIH | National Institute on Deafness and Other Communication Disorders (NIDCD)
- R01 DC011287/DC/NIDCD NIH HHS/United States
- R01 AA024103/AA/NIAAA NIH HHS/United States
- R01 AA027236/AA/NIAAA NIH HHS/United States
- U10 AA008401/AA/NIAAA NIH HHS/United States
- AA027236/HHS | NIH | National Institute on Alcohol Abuse and Alcoholism (NIAAA)
LinkOut - more resources
Full Text Sources
Medical