

Recruitment of renal functional reserve by intravenous amino acid loading in a sheep model of cardiopulmonary bypass
- PMID: 40637920
- PMCID: PMC12246334
- DOI: 10.1186/s40635-025-00774-4
Recruitment of renal functional reserve by intravenous amino acid loading in a sheep model of cardiopulmonary bypass
Abstract
Background: Cardiopulmonary bypass (CPB) may decrease the renal functional reserve (RFR). However, the temporal changes in RFR after during the recovery period after CPB remains unknown. We assessed RFR before and then weekly after CPB over four weeks following CPB in non-anaesthetised sheep.
Methods: In 10 Merino ewes, amino acids were infused before CPB and weekly for four weeks to assess RFR. At each assessment, we measured renal blood flow (RBF), renal oxygen delivery (RDO2), creatinine clearance and medullary and cortical oxygenation. Histological assessment was performed at 4 weeks.
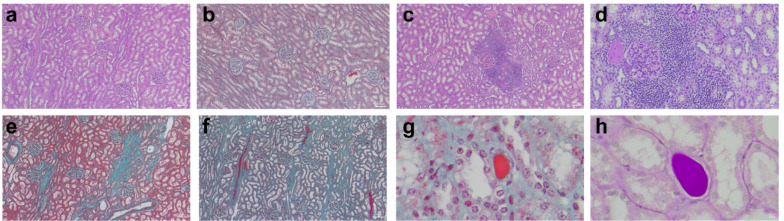
Results: Before CPB, amino acid infusion increased RBF from (mean ± SD) 6.60 ± 1.64 to 8.56 ± 1.80 mL/kg/min, and RDO2 from 0.80 ± 0.28 to 1.12 ± 0.37 mL O2/kg/min. These renal macro-circulatory responses remained consistent across all weekly assessments after CPB. Amino acid infusion also increased creatinine clearance (from 62.5 ± 15.0 to 110 ± 30.6 mL/h pre-CPB) throughout the study period. RFR remained unchanged over time (P = 0.53). However, compared with pre-CPB values, medullary (33.9 ± 9.0 pre-CPB to 15.1 ± 13.2 mmHg at 4 weeks, P = 0.0068) and cortical tissue PO2 (46.0 ± 14.2 to 17.2 ± 6.5 mmHg, P = 0.0029) decreased over time. Furthermore, the response of the medullary (but not cortical) PO₂ to amino acid infusion changed over time (P = 0.0064). While medullary PO₂ did not change in response to amino acid infusion pre-CPB and at one week after CPB, it appeared to fall from two weeks thereafter (P = 0.039 and 0.091 at weeks 2 and 3, respectively). Despite preserved RFR, sheep exposed to CPB showed greater peritubular inflammation, interstitial fibrosis and tubular casts compared with healthy controls (P = 0.007, 0.021, 0.007, respectively).
Conclusions: In this large mammalian model of CPB, weekly amino acid administration consistently recruited RFR over four weeks, despite the presence of histological injury. However, it was associated with the development of renal medullary hypoxia after two weeks. These findings highlight the complexity of the pathophysiological response of the kidney to CPB.
Keywords: Acute kidney disease; Acute kidney injury; Amino acids; Cardiac surgery; Cardiopulmonary bypass; Chronic kidney disease; Renal functional reserve.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All experimental procedures were approved by the Animal Ethics Committee of the Florey Institute of Neuroscience and Mental Health (approval number 18–119-FINMH). Consent for publication: Not applicable. Competing interests: Authors have no competing interests to disclose.
Figures




References
-
- Wang Y, Bellomo R (2017) Cardiac surgery-associated acute kidney injury: risk factors, pathophysiology and treatment. Nat Rev Nephrol 13:697–711. 10.1038/nrneph.2017.119 - PubMed
-
- Mariscalco G, Lorusso R, Dominici C et al (2011) Acute kidney injury: a relevant complication after cardiac surgery. Ann Thorac Surg 92:1539–1547. 10.1016/j.athoracsur.2011.04.123 - PubMed
-
- Cho JS, Shim J-K, Lee S et al (2021) Chronic progression of cardiac surgery associated acute kidney injury: intermediary role of acute kidney disease. J Thorac Cardiovasc Surg 161:681-688.e3. 10.1016/j.jtcvs.2019.10.101 - PubMed
-
- Ishani A, Nelson D, Clothier B et al (2011) The magnitude of acute serum creatinine increase after cardiac surgery and the risk of chronic kidney disease, progression of kidney disease, and death. Arch Intern Med 171:226–233. 10.1001/archinternmed.2010.514 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
