

Spillover of Azithromycin Mass Drug Administration and Child Survival: A Secondary Analysis of a Cluster-Randomized Clinical Trial
- PMID: 40638118
- PMCID: PMC12246876
- DOI: 10.1001/jamanetworkopen.2025.19693
Spillover of Azithromycin Mass Drug Administration and Child Survival: A Secondary Analysis of a Cluster-Randomized Clinical Trial
Abstract
Importance: World Health Organization guidelines on azithromycin mass drug administration for child survival target infants aged 1 to 11 months, although prior studies included those aged 1 to 59 months. The AVENIR trial suggested that infants aged 1 to 11 months have lower mortality if children aged 12 to 59 months in the same household are also included.
Objective: To assess the possibility of a spillover effect by examining the association of azithromycin and mortality among children aged 1 to 11 months in subgroups defined by the presence of a child aged 12 to 59 months in the same household.
Design, setting, and participants: This exploratory secondary analysis of the AVENIR (Azithromycine Pour la Vie des Enfants au Niger: Implementation et Recherche) adaptive cluster-randomized clinical trial was performed in 3000 rural and periurban communities in Niger. AVENIR communities were randomized to 3 arms and followed up for 2 years (November 24, 2020, to July 31, 2023). Study arms consisted of children aged 1 to 59 months receiving azithromycin (child arm); infants aged 1 to 11 months receiving azithromycin with placebo to children aged 12 to 59 months (infant arm); and children aged 1 to 59 months receiving placebo (placebo arm). Participants, investigators, data collectors, and data analysts were masked to randomization.
Intervention: A single 20-mg/kg dose of oral azithromycin or placebo administered by study staff biannually.
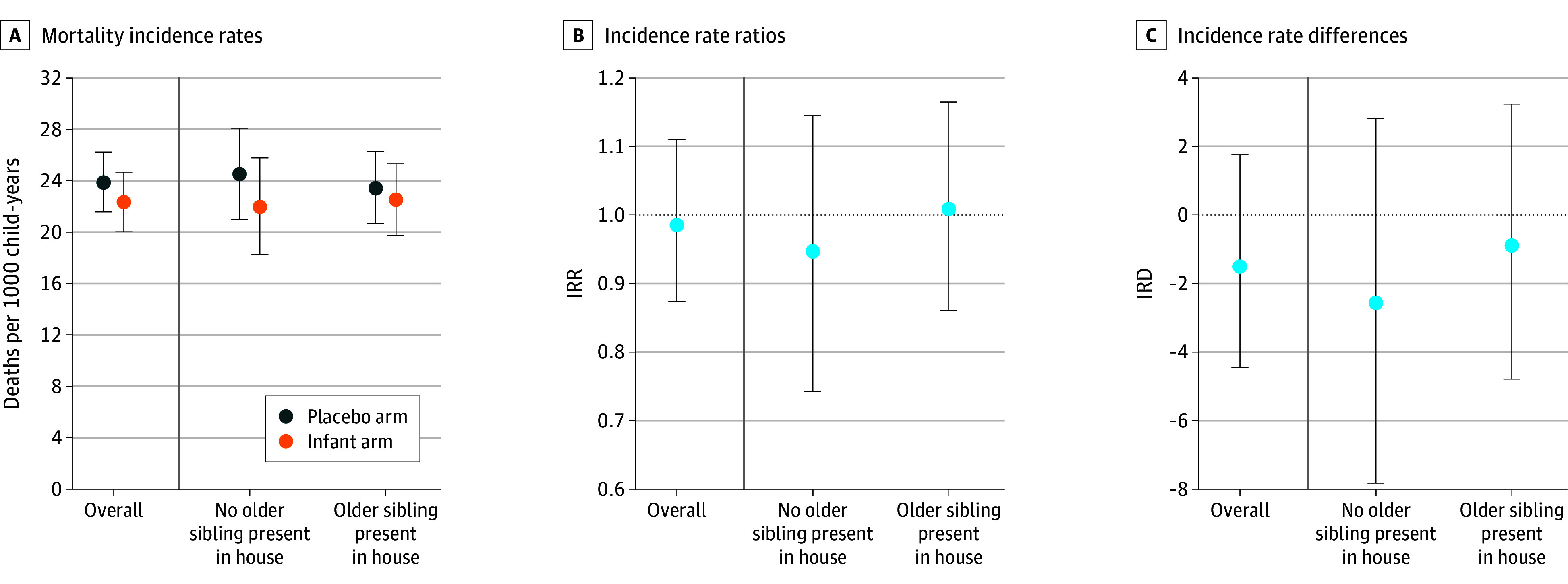
Main outcomes and measures: All-cause mortality in infants aged 1 to 11 months (deaths per 1000 person-years) measured through biannual census. Subgroups were defined by the presence of a child aged 12 to 59 months in the household recorded during the census.
Results: After exclusions, 2883 communities and 98 969 infants aged 1 to 11 months were included in the analysis. Among the 23 770 infants in allocation 1 at baseline, mean (SD) age was 6.2 (3.1) months and 11 974 (50.4%) were female. Mortality was 18.5 (95% CI, 16.7-20.4) deaths per 1000 person-years in the child arm, 22.3 (95% CI, 20.0-24.7) in the infant arm, and 23.9 (95% CI, 21.6-26.2) in the placebo arm. The incidence rate ratio comparing mortality in the child and infant arms among children with an older sibling was 0.78 (95% CI, 0.65-0.93) compared with 0.91 (95% CI, 0.73-1.15; P = .26 for interaction) among those without. Comparing the infant and placebo arms, the incidence rate ratio among children with an older sibling was 0.96 (95% CI, 0.81-1.14) compared with 0.90 (95% CI, 0.71-1.12; P = .61 for interaction) among those without.
Conclusions and relevance: In this secondary analysis of a cluster-randomized clinical trial, interaction for the presence of a older sibling was not statistically significant, but results were consistent with lower mortality among infants aged 1 to 11 months living with older, treated children.
Trial registration: ClinicalTrials.gov Identifier: NCT04224987.
Conflict of interest statement
Figures


Similar articles
-
Mass distribution of azithromycin and child mortality among underweight infants in rural Niger: a subgroup analysis of the AVENIR cluster-randomised trial.BMJ Open. 2025 Mar 27;15(3):e097916. doi: 10.1136/bmjopen-2024-097916. BMJ Open. 2025. PMID: 40147984 Free PMC article. Clinical Trial.
-
Biannual Mass Azithromycin Distributions for Preschool Children and Malaria Parasitemia: A Secondary Analysis of the MORDOR Cluster Randomized Trial.JAMA Netw Open. 2025 Aug 1;8(8):e2527148. doi: 10.1001/jamanetworkopen.2025.27148. JAMA Netw Open. 2025. PMID: 40824641 Free PMC article.
-
Safety and efficacy of repeat ivermectin mass drug administrations for malaria control (RIMDAMAL II): a phase 3, double-blind, placebo-controlled, cluster-randomised, parallel-group trial.Lancet Infect Dis. 2025 Jul;25(7):737-750. doi: 10.1016/S1473-3099(24)00751-5. Epub 2025 Feb 4. Lancet Infect Dis. 2025. PMID: 39919778 Clinical Trial.
-
Macrolide antibiotics (including azithromycin) for cystic fibrosis.Cochrane Database Syst Rev. 2024 Feb 27;2(2):CD002203. doi: 10.1002/14651858.CD002203.pub5. Cochrane Database Syst Rev. 2024. PMID: 38411248 Free PMC article.
-
Antibiotics for trachoma.Cochrane Database Syst Rev. 2011 Mar 16;(3):CD001860. doi: 10.1002/14651858.CD001860.pub3. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2019 Sep 26;9:CD001860. doi: 10.1002/14651858.CD001860.pub4. PMID: 21412875 Updated.
References
-
- World Health Organization . WHO Guideline on Mass Drug Administration of Azithromycin to Children Under Five Years of Age to Promote Child Survival. World Health Organization; 2020. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
