

The triglyceride-glucose index, a marker of insulin resistance, as a predictor of thrombotic risk in atrial fibrillation
- PMID: 40640827
- PMCID: PMC12247220
- DOI: 10.1186/s12933-025-02809-2
The triglyceride-glucose index, a marker of insulin resistance, as a predictor of thrombotic risk in atrial fibrillation
Abstract
Background: Atrial fibrillation (AF) increases the risk of stroke making accurate risk stratification central for effective management. The triglyceride-glucose (TyG) index, a marker of insulin resistance, has been associated to cardiovascular diseases. Indeed, it is particularly relevant in the context of diabetes and metabolic syndrome, which are major contributors to cardiovascular risk. Herein, we explored whether the TyG index could predict thrombotic events in AF patients.
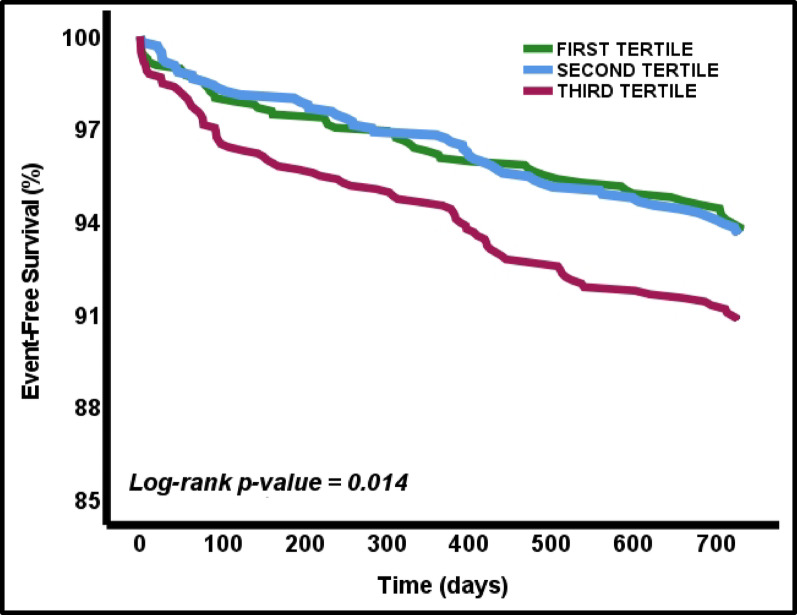
Methods: Prospective cohort study involving AF outpatients starting oral anticoagulation (OAC) therapy between January 2016 and November 2021. The primary endpoint was a composite of thrombotic events including myocardial infarction, venous thromboembolism, ischemic stroke, or transient ischemic attack, over 2 years follow-up. The TyG index was calculated at baseline and patients were stratified into tertiles (T1: TyG index < 4.59; T2: TyG index 4.59–4.83; T3: TyG index > 4.83).
Results: 2907 patients (52.5% women; median age 77 years, IQR 69–82 years) were included, with a median TyG index of 4.71 (4.53–4.91). At 2-years, 7.2% (208) of patients experienced a composite thrombotic event. Patients in T3 had a significantly higher incidence rate ratio (1.39 [95% CI 1.01–1.96], p = 0.047 vs. T1; 1.42 [95% CI 1.01–2.00], p = 0.038 vs. T2). Adjusted Cox regression identified the TyG index as an independent predictor for thrombotic events (aHR 1.82; 95% CI 1.15–2.89). T3 patients exhibited a 64% higher risk of thrombotic events (aHR 1.64, 95% CI 1.17–2.29; log-rank test p value = 0.014).
Conclusions: In this real-world cohort of AF patients on OAC, an elevated TyG index independently predicted thrombotic events. However, further research is needed to determine how to integrate this simple marker into existing risk stratification strategies and whether it truly improves risk assessment and treatment decisions.
Supplementary Information: The online version contains supplementary material available at 10.1186/s12933-025-02809-2.
Keywords: Atrial fibrillation; Risk prediction; Stroke; Triglyceride-glucose index.
Conflict of interest statement
Declarations. Competing interests: Gregory Y.H. Lip: consultant and speaker for BMS/Pfizer, Boehringer Ingelheim, Daiichi-Sankyo, Anthos. No fees are received personally. He is a National Institute for Health and Care Research (NIHR) Senior Investigator and co-principal investigator of the AFFIRMO project on multimorbidity in AF, which has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No. 899871. José Miguel Rivera-Caravaca: Consultant for Idorsia Pharmaceuticals LTD. Francisco Marín is consultant and speaker for Boehringer-Ingelheim and BMS/Pfizer. There is nothing to disclose for other authors.
Figures


References
-
- Kezerle L, Tsadok MA, Akriv A, Senderey AB, Bachrach A, Leventer-Roberts M, et al. Pre-diabetes increases stroke risk in patients with nonvalvular atrial fibrillation. J Am Coll Cardiol. 2021;77(7):875–84. - PubMed
-
- Esteve-Pastor MA, Rivera-Caravaca JM, Roldán-Rabadán I, Roldán V, Muñiz J, Raña-Míguez P, et al. Quality of oral anticoagulation with vitamin K antagonists in “real-world” patients with atrial fibrillation: a report from the prospective multicentre FANTASIIA registry. Europace. 2018;20(9):1435–41. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
