

Critical care, critical gaps: assessment of burnout and behavioral profiles of ICU healthcare workers in China-a multicenter cross-sectional study
- PMID: 40642244
- PMCID: PMC12240766
- DOI: 10.3389/fpubh.2025.1617081
Critical care, critical gaps: assessment of burnout and behavioral profiles of ICU healthcare workers in China-a multicenter cross-sectional study
Abstract
Background: Burnout in intensive care unit (ICU) healthcare workers (HCWs) is a persistent threat to patient safety and workforce stability. While most evidence is derived from crisis settings, the behavioral determinants of burnout in routine, post-pandemic ICUs remain under-explored. This study applies a Knowledge-Attitude-Practice (KAP) framework to assess burnout-related KAP and identify its demographic, occupational, and institutional predictors.
Methods: In this cross-sectional study, 4,500 eligible ICU healthcare workers (HCWs) from 10 facilities in Yancheng, Jiangsu, China, were invited to complete a rigorously validated KAP survey; 3,342 responded (response rate = 74.3%), with KR-20 = 0.87 for Knowledge and Cronbach's α ≥ 0.82 for Attitude and Practice. Descriptive statistics summarized participant characteristics, and multivariable logistic regression identified predictors of adequate (≥75%) KAP profiles.
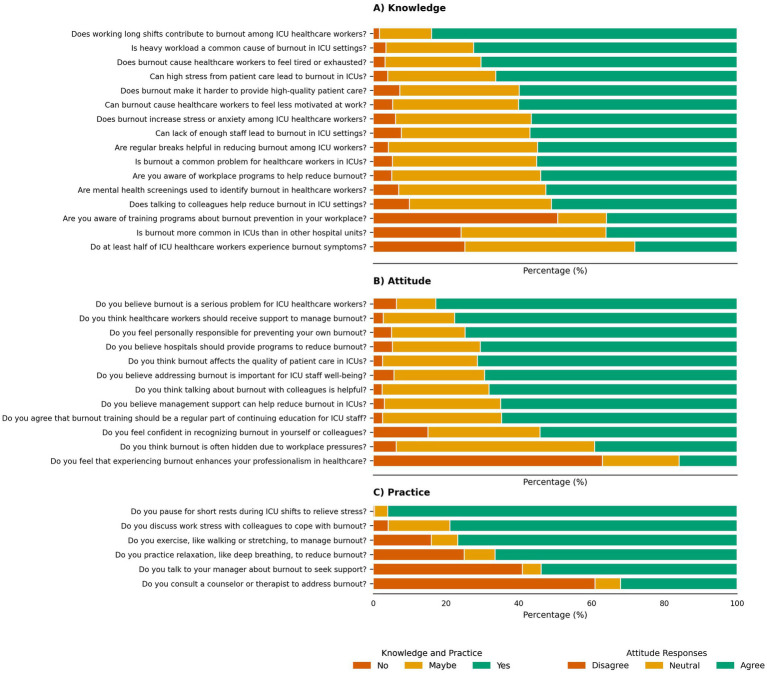
Results: The cohort was predominantly female (70%) and nurse-dominated (60%). Most respondents identified long shifts (84.0%) and heavy workloads (72.4%) as principal burnout drivers, yet only 35.9% were aware of formal prevention programs. Although 82.8% perceived burnout as a serious threat and 74.7% assumed personal responsibility, formal mitigation remained sparely 53.8% sought managerial support and 39.0% ever accessed counseling. Informal coping was pervasive: breaks (96.0%), peer discussion (78.9%), and exercise (76.8%). Access to workplace mental health resources was reported by 40.0%, with 50.0% reporting no access and 10.0% unsure, strongly predicting higher knowledge (adjusted OR 4.01, 95% CI 3.35-4.80) and good practice (OR 4.01, 95% CI 3.35-4.80). Clinical role, mid-career status, and 1-10 years' ICU experience independently improved KAP scores (ORs 3.98-6.00, p < 0.001), whereas contract and temporary staff were consistently disadvantaged (OR 0.54, 95% CI 0.42-0.70). Gender, marital status, and ICU type were non-significant.
Conclusion: Burnout in ICU HCWs persists as a structural-behavioral challenge post-pandemic. Interventions should prioritize institutional support, equitable mental health access, and inclusion of vulnerable groups. This study shows the KAP model's role in crafting scalable, data-driven prevention strategies for critical care.
Keywords: KAP survey; burnout; healthcare workers; intensive care; mental-health resources; workforce resilience.
Copyright © 2025 Zhang, Li, He, Xu, Wu, He, Wang and Lu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Stocchetti N, Segre G, Zanier ER, Zanetti M, Campi R, Scarpellini F, et al. Burnout in intensive care unit workers during the second wave of the COVID-19 pandemic: a single center cross-sectional Italian study. Int J Environ Res Public Health. (2021) 18:6102. doi: 10.3390/ijerph18116102, PMID: - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical