

Medical Thoracoscopy in Malignant Pleural Effusion
- PMID: 40642715
- PMCID: PMC12244283
- DOI: 10.7759/cureus.85707
Medical Thoracoscopy in Malignant Pleural Effusion
Abstract
Introduction: Malignant pleural effusion (MPE) is a common complication of advanced malignancies, often resulting in significant morbidity and impaired quality of life. In most cases, pleural fluid cytology remains negative. In the era of targeted cancer therapy, pathologists expect larger tissue samples. Therefore, medical thoracoscopy (MT) has gained popularity for adequate tissue sampling under supervision. During MT, various morphological pleural lesions were identified, yet their histopathological associations remain unknown. This study aimed to assess the diagnostic yield of medical thoracoscopy and the complications associated with the procedure. We also observed various morphological lesions in MPE and their histopathological associations.
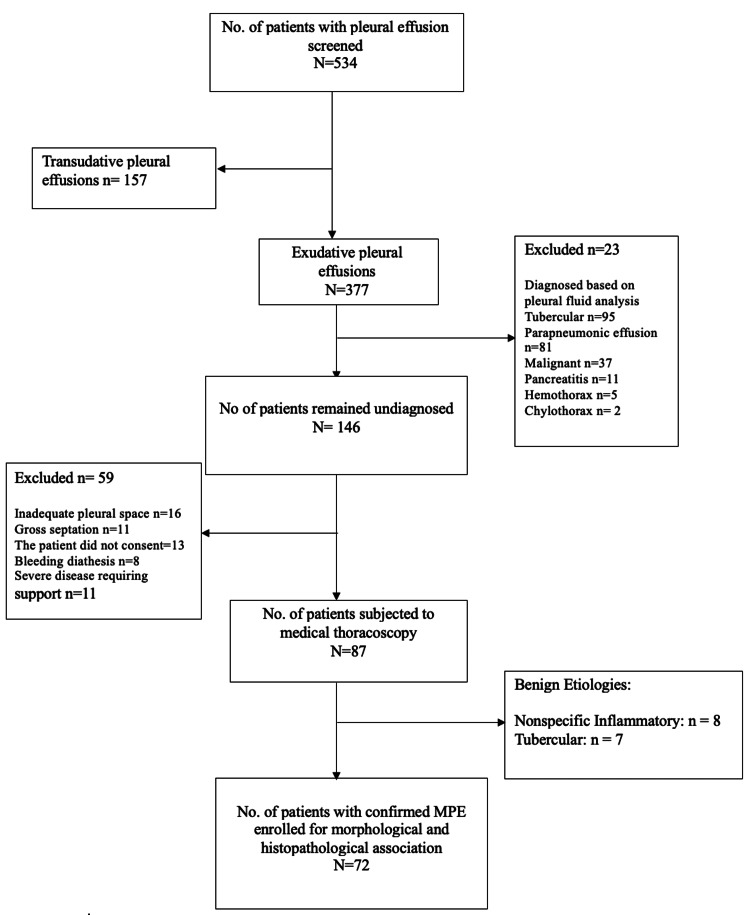
Methods: This was a single-center, hospital-based, prospective cross-sectional study conducted in the Department of Pulmonary Medicine, Veer Surendra Sai Institute of Medical Sciences and Research (VIMSAR), Burla, India. Patients with undiagnosed pleural effusion underwent MT. During the procedure, the lesions were morphologically characterized, and samples were collected for histopathological examination (HPE).
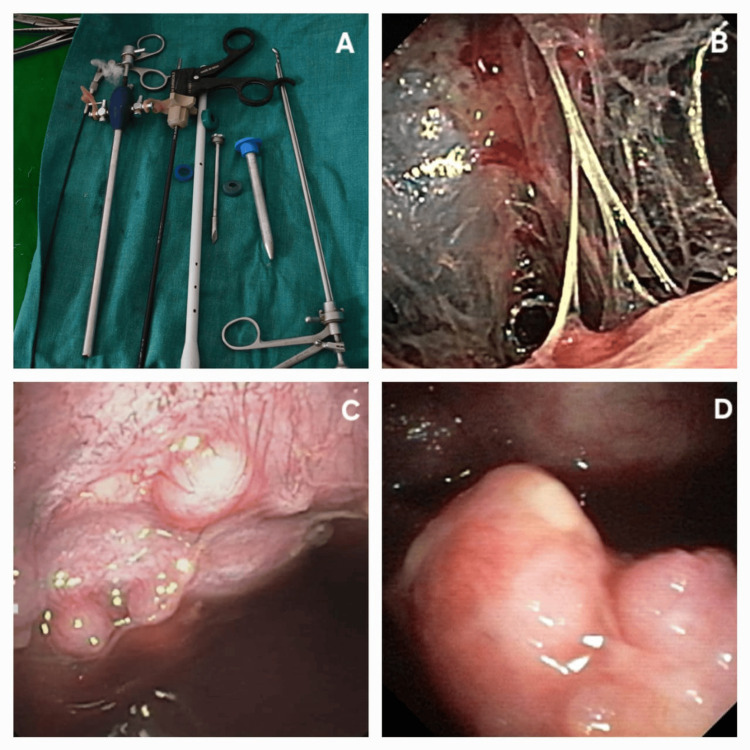
Results: A total of 87 patients underwent medical thoracoscopy using a rigid thoracoscope (Optymed®, Delhi, India), out of which 72 patients had malignant effusion and seven patients had tuberculous effusion. Eight patients had nonspecific inflammation. The diagnostic yield of medical thoracoscopy in this study was at least 90.8% (95% CI: 84.8%-96.8%). Seventy-two patients were evaluated for histopathologic and morphologic association. The most common procedure-related complication was pain at the incision site (87, 100%, median Visual Analogue Scale (VAS): 5), followed by desaturation. The mean fall in saturation was 5.13% (±33.78%). We did not observe any serious adverse effects related to rigid MT. The mean age of the patients was 54.17 (±15.17) years. Among MPE, pleural-based nodules (46, 63.9%), followed by adhesions (27, 37.5%), were the most common findings during MT. Other noted lesions included masses (26, 36.12%), plaques (22, 30.56%), and strands (19, 26.39%). Nodules were significantly associated with metastatic adenocarcinoma (p<0.01). Adhesions and plaques were commonly linked with pleural abnormalities in malignant mesothelioma (p<0.01). Masses were most frequently associated with lymphomas (p<0.01) and undifferentiated carcinoma (p<0.01). Small cell carcinoma comprised only five patients among MPE and was associated with strands (p<0.01).
Conclusion: Medical thoracoscopy is a valuable tool in evaluating and managing malignant pleural effusion. Its high diagnostic accuracy, therapeutic capabilities, and favorable safety profile make it the procedure of choice in appropriate clinical settings. Specific morphological patterns may be observed in different pleural malignancies.
Keywords: malignant pleural effusion; mass; medical thoracoscopy; nodule; plaque.
Copyright © 2025, Rath et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Veer Surendra Sai Institute of Medical Science and Research (VIMSAR) Institute of Research and Ethics Committee (VIREC) issued approval 2015/P-I-RP/131. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Five-year Experience of Using Single Port Rigid Thoracoscopy in Patients of Undiagnosed Exudative Pleural Effusion at Tertiary Center in North India.Ann Afr Med. 2025 Jun 27. doi: 10.4103/aam.aam_70_25. Online ahead of print. Ann Afr Med. 2025. PMID: 40576394 English, French.
-
Interventions for the management of malignant pleural effusions: a network meta-analysis.Cochrane Database Syst Rev. 2016 May 8;2016(5):CD010529. doi: 10.1002/14651858.CD010529.pub2. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2020 Apr 21;4:CD010529. doi: 10.1002/14651858.CD010529.pub3. PMID: 27155783 Free PMC article. Updated.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Does Augmenting Irradiated Autografts With Free Vascularized Fibula Graft in Patients With Bone Loss From a Malignant Tumor Achieve Union, Function, and Complication Rate Comparably to Patients Without Bone Loss and Augmentation When Reconstructing Intercalary Resections in the Lower Extremity?Clin Orthop Relat Res. 2025 Jun 26. doi: 10.1097/CORR.0000000000003599. Online ahead of print. Clin Orthop Relat Res. 2025. PMID: 40569278
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
References
-
- The undiagnosed pleural effusion. Light RW. Clin Chest Med. 2006;27:309–319. - PubMed
-
- Etiology and prognostic significance of massive pleural effusions. Jiménez D, Díaz G, Gil D, Cicero A, Pérez-Rodríguez E, Sueiro A, Light RW. Respir Med. 2005;99:1183–1187. - PubMed
-
- Diagnostic sensitivity of pleural fluid cytology in malignant pleural effusions: systematic review and meta-analysis. Kassirian S, Hinton SN, Cuninghame S, et al. Thorax. 2023;78:32–40. - PubMed
-
- Medical thoracoscopy/pleuroscopy: step by step. Loddenkemper R, Lee P, Noppen M, Mathur PN. Breathe. 2011;8:156–167.
LinkOut - more resources
Full Text Sources