

Evaluating long-term outcomes and the impact of small aortic annulus on valve replacement-a novel systematic review and meta-analysis comparing surgery vs. transcatheter interventions
- PMID: 40642752
- PMCID: PMC12241089
- DOI: 10.3389/fcvm.2025.1555853
Evaluating long-term outcomes and the impact of small aortic annulus on valve replacement-a novel systematic review and meta-analysis comparing surgery vs. transcatheter interventions
Abstract
Background: Transcatheter aortic valve implantation (TAVI) is often compared to surgical aortic valve replacement (SAVR) for aortic stenosis treatment. This meta-analysis evaluates the long-term efficacy and safety of TAVI vs. SAVR in aortic stenosis patients, as well as their respective impact on patients with small aortic annulus (SAA).
Methods: MEDLINE, Embase, Cochrane Library, and ClinicalTrials.gov were searched for randomized controlled trials (RCTs) and comparative observational studies on TAVI vs. SAVR with long-term follow-up (3-5 years) or SAA. Risk of bias was assessed using the Cochrane Risk of Bias tool (RoB 2.0) and the Newcastle Ottawa Scale. Meta-analyses were conducted with RevMan 5.4 using a random-effects model, with risk ratio (RR) and mean difference (MD) as effect measures.
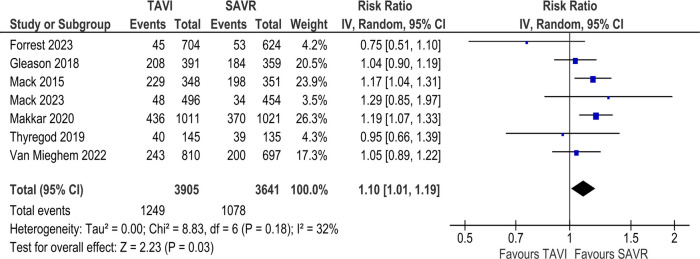
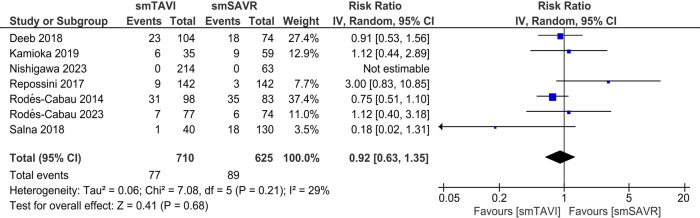
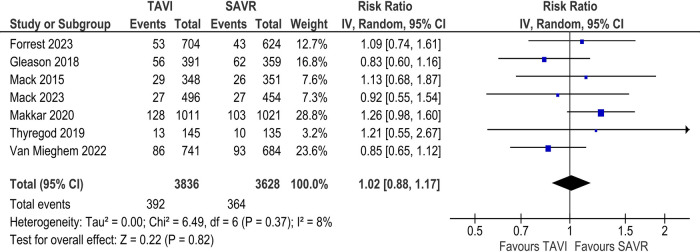
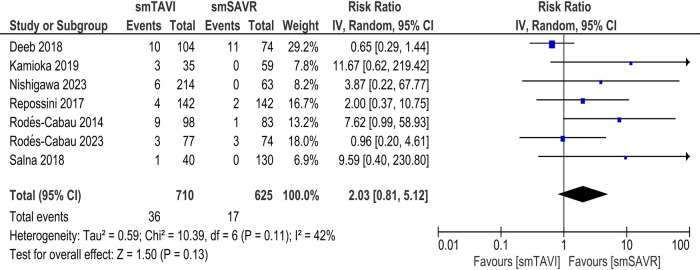
Results: A total of 17 studies were included in our review. In the long-term analysis, all-cause mortality was significantly higher in the TAVI group [RR 1.10; 95% CI: 1.01-1.19], but the incidence of major bleeding [RR 0.79; 95% CI: 0.68-0.90] and atrial fibrillation was significantly lower [RR 0.37; 95% CI: 0.29-0.48] in the TAVI group. No significant difference was found between the two groups regarding other long-term outcomes. For SAA outcomes, there was no significant difference in terms of all-cause mortality [RR 0.92; 95% CI: 0.63-1.35], although cardiovascular mortality was significantly increased in the TAVI group [RR 2.08; 95% CI: 1.09-3.98]. TAVI significantly increased the rate of major vascular complications [RR 3.58; 95% CI: 1.10-11.61], aortic regurgitation/PVL [RR 6.91; 95% CI: 2.66-17.97], and pacemaker implantation (RR 2.87; 95% CI: 1.74-4.75]. TAVI significantly improved the incidence of prosthesis patient mismatch [RR 0.70; 95% CI: 0.54-0.89], effective orifice valve area (EOA) [MD 0.10; 95% CI: 0.01-0.19], and length of stay in hospital [MD -4.88; 95% CI: -5.52 to -4.23]. There were no significant differences in other clinical or echocardiographic outcomes.
Conclusions: TAVI was associated with higher long-term all-cause mortality compared to SAVR in the overall population. Among patients with small aortic annulus, no survival benefit was observed with TAVI, and cardiovascular mortality was significantly increased. Future RCTs should explore SAA-related outcomes with standardized diagnostic criteria.
Systematic review registration: https://www.crd.york.ac.uk, PROSPERO CRD42024541862.
Keywords: SAVR; TAVI; TAVR—transcatheter aortic valve replacement; small aortic annulus; transcatheter and surgical aortic valve replacement.
© 2025 Amin, Mohammed, Kajitani, AlMashari, Kumar, Sabir, Briz-Echeverria, Mokhtassi, Kallikere Lakshmana, Bokhari, Ehsan, Ahmad, Ahmed and Bahrami.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Meta-analysis of longitudinal comparison of transcatheter versus surgical aortic valve replacement in patients at low to intermediate surgical risk.Int J Surg. 2024 Dec 1;110(12):8097-8106. doi: 10.1097/JS9.0000000000002158. Int J Surg. 2024. PMID: 39806748 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Transcatheter aortic valve implantation for aortic stenosis in high surgical risk patients: A systematic review and meta-analysis.PLoS One. 2018 May 10;13(5):e0196877. doi: 10.1371/journal.pone.0196877. eCollection 2018. PLoS One. 2018. PMID: 29746546 Free PMC article.
-
Transcatheter Versus Surgical Approach for the Treatment of Aortic Stenosis in Patients With Concomitant Coronary Artery Disease: A Systematic Review and Meta-Analysis.Catheter Cardiovasc Interv. 2025 Jul 1. doi: 10.1002/ccd.31697. Online ahead of print. Catheter Cardiovasc Interv. 2025. PMID: 40590217 Review.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
References
-
- Baron SJ, Arnold SV, Wang K, Magnuson EA, Chinnakondepali K, Makkar R, et al. Health status benefits of transcatheter vs. surgical aortic valve replacement in patients with severe aortic stenosis at intermediate surgical risk: results from the PARTNER 2 randomized clinical trial. JAMA Cardiol. (2017) 2(8):837–45. 10.1001/jamacardio.2017.2039 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources