

Lab efficiency and improvements in the management of bloodstream infections: a before and after study
- PMID: 40643849
- PMCID: PMC12484295
- DOI: 10.1007/s10096-025-05200-x
Lab efficiency and improvements in the management of bloodstream infections: a before and after study
Abstract
Purpose: Early availability of identification of bacterial pathogens and knowledge of their antimicrobial susceptibility is crucial when managing patients with bloodstream infections (BSI). We aimed to assess the impact of the laboratory conversion (full automation and conversion to 24/7 workflow) on laboratory efficiency, timeliness of diagnostic results, and patient outcomes.
Methods: An observational retrospective study was conducted to compare lab organisation, laboratory times including turnaround time (TAT) for positive blood cultures (PBCs), antimicrobial therapy (antibiotic prescription, time to first antibiotic modification), patient outcomes (30-day mortality, hospital and ICU discharge), and antibiotic consumption for pre- and post-conversion periods (January to December 2019 versus June 2021 to May 2022) in adults with BSI admitted to the ICU at the Centre Hospitalier de Valenciennes. Multivariable models were used to compare periods, adjusting for relevant patient characteristics.
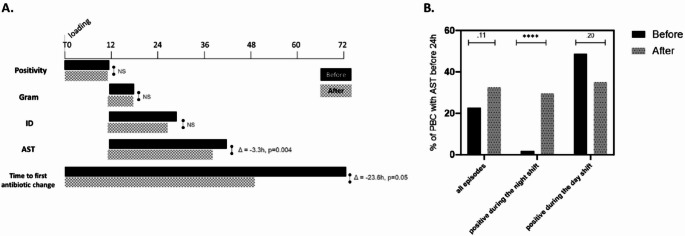
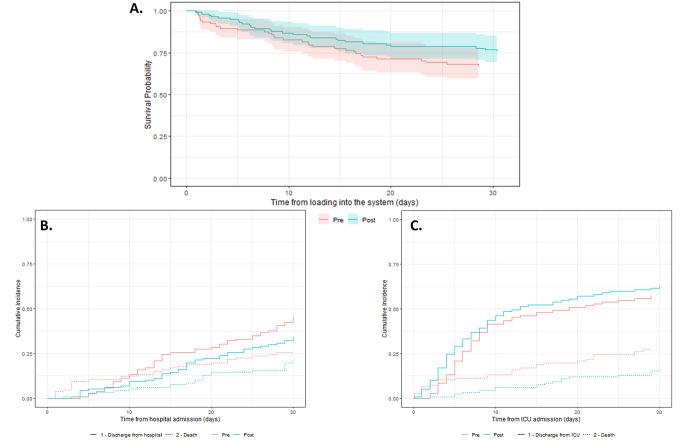
Results: A total of 116 and 128 PBCs from 104 to 112 patients in pre- and post-conversion were analysed. TAT decreased significantly for clinically significant episodes (median 30.4 (n = 83) versus 27.1 h (n = 84), p = 0.004). The percent of PBCs with antimicrobial susceptibility testing results available within 24 h increased significantly for night shift PBCs (0.9% versus 18.7%; p < 0.0001). A significant reduction in time to first antibiotic modification occurred (median difference of 19.1 h, p = 0.04). Additionally, we observed for the post-conversion a 51% increase in probability of ICU discharge (hazard ratio [HR] = 1.51, 95%CI 1.09‒2.08, p = 0.014) and a trend towards a reduction in 30-day mortality (HR = 0.65, 95%CI 0.40‒1.06, p = 0.085).
Conclusion: Laboratory reorganisation improved laboratory efficiency, leading to improvements in the management of patients with BSIs.
Clinical Trial Number: Not applicable.
Supplementary Information: The online version contains supplementary material available at 10.1007/s10096-025-05200-x.
Keywords: Antimicrobial stewardship; Bloodstream infections; Efficiency; Lab automation.
Conflict of interest statement
Declarations. Ethical approval: This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Clinical Research Ethics Commission (CERCI) of the Valenciennes Hospital (24/03/2022/No CHV-2022-008). Human ethics and consent to participate: Informed consent was obtained from all individual participants included in the study. Competing interests: Eric Rethore, Arnaud Dubrulle and Lélia Abad are employees of bioMérieux. The remaining authors have no relevant financial or non-financial interests to disclose.
Figures
References
-
- Maurer FP, Christner M, Hentschke M, Rohde H (2017) Advances in rapid identification and susceptibility testing of Bacteria in the clinical microbiology laboratory: implications for patient care and antimicrobial stewardship programs. Infect Dis Rep 9(1):6839. 10.4081/idr.2017.6839 - DOI - PMC - PubMed
-
- Trigueiro G, Oliveira C, Rodrigues A, Seabra S, Pinto R, Bala Y, Gutierrez Granado M, Vallejo S, Gonzalez V, Cardoso C (2024) Conversion of a classical microbiology laboratory to a total automation laboratory enhanced by the application of lean principles. Microbiol Spectr 12(2):e0215323. 10.1128/spectrum.02153-23 - DOI - PMC - PubMed
-
- Bou G, Calbo E, Crespo M, Canton R, Alvarez de Luna FF, Garcia Rodriguez J, Angel Goenaga M, Gonzalez-Garcia J, Gonzalez J, Larrosa N, Martinez-Martinez L, Navarro D, Ramon Pano J, Rivero A, Carlos Rodriguez J, Tomas M, Vilaj J (2022) Justification for 24/7 clinical microbiology services. Enferm Infecc Microbiol Clin (Engl Ed) 40(1):1–4. 10.1016/j.eimce.2021.08.014 - DOI - PubMed
-
- SPILF (2022) Actualisation de la liste des antibiotiques critiques disponibles en France pour l’exercice libéral ET en établissements de santé, https://www.infectiologie.com/UserFiles/File/spilf/recos/saisine-dgs-atb...
LinkOut - more resources
Full Text Sources
Miscellaneous
