

Savings Associated With Bundled Payments for Outpatient Spine Surgery Among Medicare Beneficiaries
- PMID: 40643923
- PMCID: PMC12254892
- DOI: 10.1001/jamahealthforum.2025.1907
Savings Associated With Bundled Payments for Outpatient Spine Surgery Among Medicare Beneficiaries
Abstract
Importance: Few value-based payment programs have targeted outpatient surgery, although these procedures comprise most surgeries performed in hospitals. In 2018, the Centers for Medicare and Medicaid Services introduced Bundled Payments for Care Improvement Advanced (BPCI Advanced), the first episode-based payment model to include an outpatient surgical condition-spine surgery. It is not known whether bundled payments reduce spending or improve quality for outpatient surgery, despite plans to expand outpatient episodes in future models.
Objective: To determine whether hospital participation in the first year of BPCI Advanced for outpatient and inpatient spine surgery (back and neck except spinal fusion procedures [BNESF]) was associated with changes in spending and quality.
Design, setting, and participants: A retrospective cohort study using Medicare claims and differences-in-differences analysis adjusting for patient and market characteristics was conducted comparing outcomes for patients receiving outpatient and inpatient BNESF from hospitals that participated in BPCI Advanced vs those receiving these procedures from a matched comparison group of nonparticipating hospitals. Medicare beneficiaries receiving outpatient and inpatient BNESF between 2013 and 2019 were included. Analyses were conducted between March 2023 and February 2024.
Exposures: Hospital participation in BPCI Advanced.
Main outcomes and measures: The primary outcome was total episode spending, including spending incurred for the index procedure and 90-day follow-up period. Secondary outcomes included 90-day return inpatient admissions, emergency department visits, and mortality.
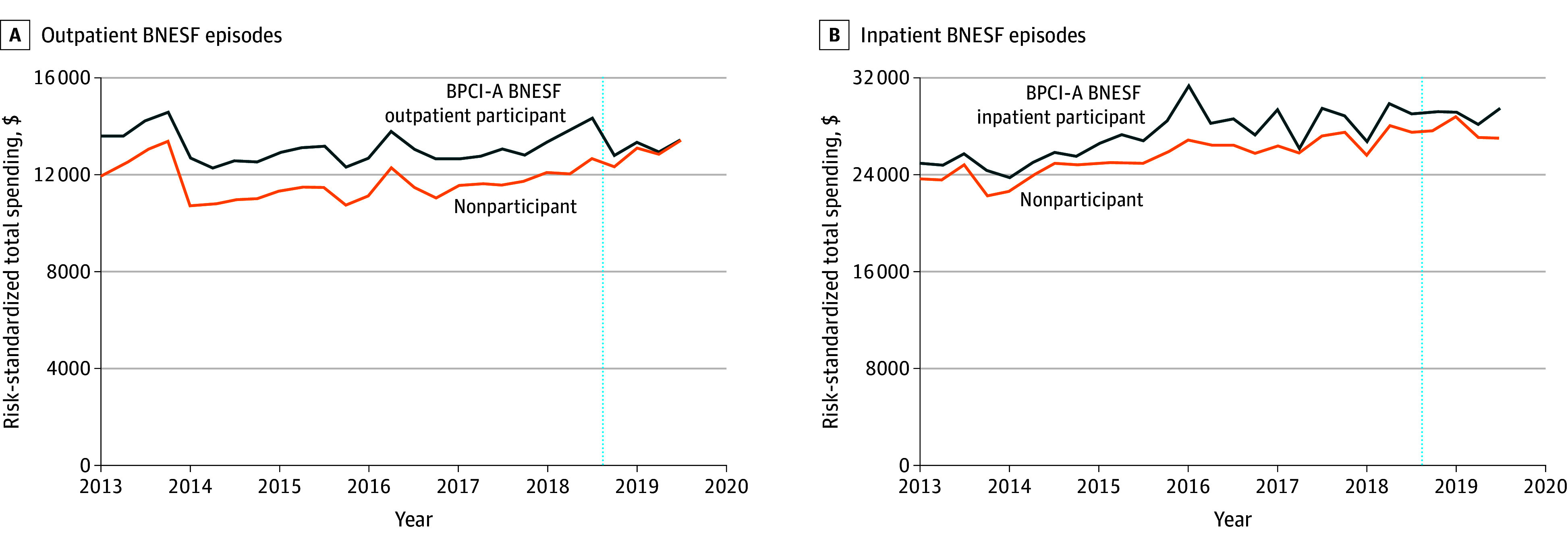
Results: Among 14 280 patients who received outpatient BNESF, hospital participation in BPCI Advanced was associated with a differential reduction in total episode spending (-$1201; 95% CI, -2184 to -219) and return inpatient admissions (-2.2 percentage points; 95% CI, -4.2 to -0.1). For outpatient procedures, the mean (SD) age was 71.8 (8.6) years; 43.9% were women, 3.9% were Black; and 3.2% were Hispanic. Among 23 440 patients who received inpatient BNESF, hospital participation in BPCI Advanced was not associated with differential changes in total episode spending or return inpatient admissions. There were no significant changes for emergency department visits or mortality for either group.
Conclusions and relavance: In this cohort study, participation in the first year of a bundled payment program for outpatient spine surgery was associated with nearly 10% lower spending. No changes in spending were observed for similar inpatient spine surgery procedures. Further evaluation of bundled payments for outpatient surgical conditions and associated changes in care delivery is needed to inform plans to include these episodes in future models.
Conflict of interest statement
Figures
Similar articles
-
Physician and Hospital Performance in Medicare's Updated Bundled-Payment Model for Joint Replacement.JAMA Health Forum. 2025 Jul 3;6(7):e251930. doi: 10.1001/jamahealthforum.2025.1930. JAMA Health Forum. 2025. PMID: 40711779
-
Medical and Surgical Episodes Among Hospital Participants in the Bundled Payments for Care Improvement-Advanced Program.JAMA Netw Open. 2024 Dec 2;7(12):e2451792. doi: 10.1001/jamanetworkopen.2024.51792. JAMA Netw Open. 2024. PMID: 39714840 Free PMC article.
-
Are Quality Scores in the Centers for Medicaid and Medicare Services Merit-based Incentive Payment System Associated With Outcomes After Outpatient Orthopaedic Surgery?Clin Orthop Relat Res. 2024 Jul 1;482(7):1107-1116. doi: 10.1097/CORR.0000000000003033. Epub 2024 Mar 21. Clin Orthop Relat Res. 2024. PMID: 38513092 Free PMC article.
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
References
-
- Steiner CA, Karaca Z, Moore BJ, Imshaug MC, Pickens G. Surgeries in Hospital-Based Ambulatory Surgery and Hospital Inpatient Settings, 2014. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Agency for Healthcare Research and Quality (US); 2006. Accessed January 26, 2024. https://www.ncbi.nlm.nih.gov/books/NBK442035/ - PubMed
-
- Hall MJ, Schwartzman A, Zhang J, Liu X. Ambulatory surgery data from hospitals and ambulatory surgery centers: United States, 2010. Natl Health Stat Report. 2017;(102):1-15. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
