

Global burden and risk factors of peptic ulcer disease between 1990 and 2021: An analysis from the global burden of disease study 2021
- PMID: 40644423
- PMCID: PMC12250541
- DOI: 10.1371/journal.pone.0325821
Global burden and risk factors of peptic ulcer disease between 1990 and 2021: An analysis from the global burden of disease study 2021
Abstract
Background: Peptic ulcer disease (PUD) is a chronic gastrointestinal disorder that may present acutely due to complications and poses significant clinical and economic challenges. Understanding the global burden of PUD and its contributing risk factors is essential for developing targeted prevention strategies. Therefore, our research aimed to comprehensively evaluate the epidemiological characteristics and associated risk factors of PUD, thereby providing evidence to support policymakers in formulating appropriate health policies.
Methods: The data on PUD were retrieved from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2021. Incidence, prevalence, deaths and disability-adjusted life years (DALYs) were metrics used to measure PUD burden. The population attributable fractions (PAFs) were used to calculate the percentage contributions of primary potential risk factors to PUD deaths and DALYs.
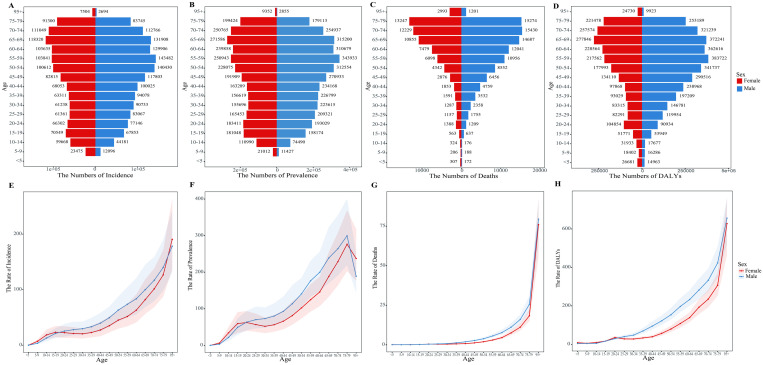
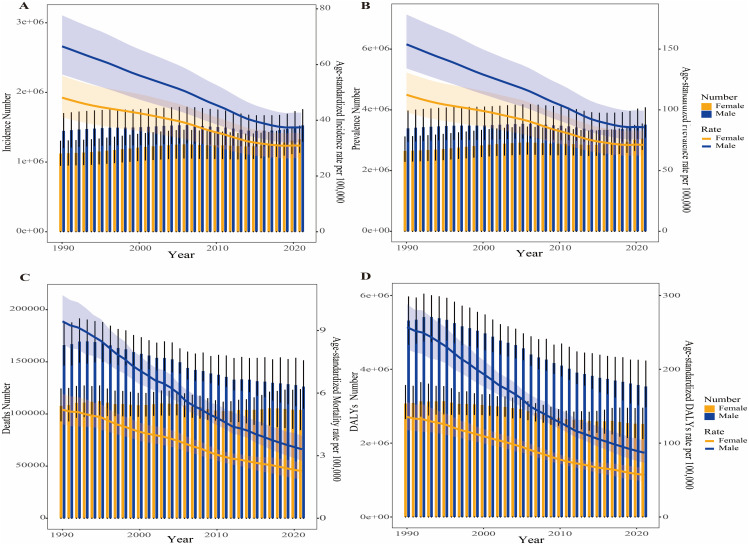
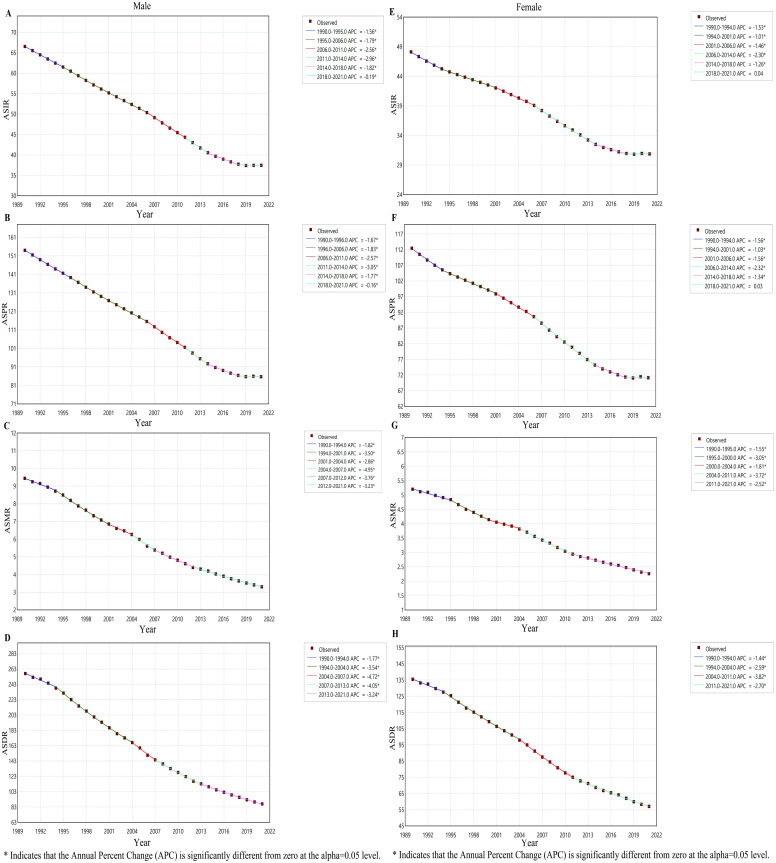
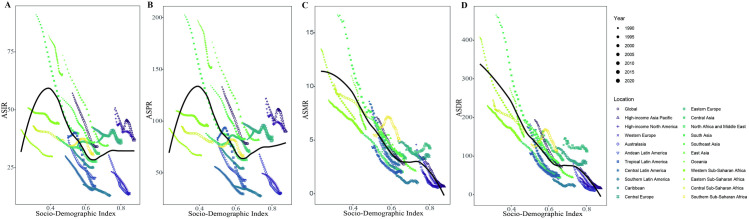
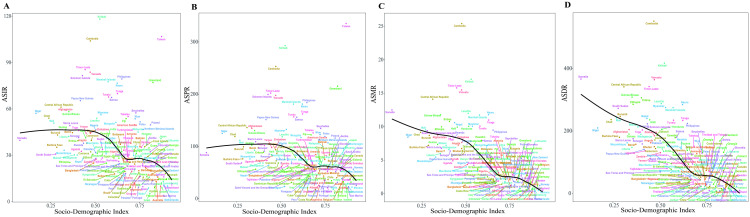
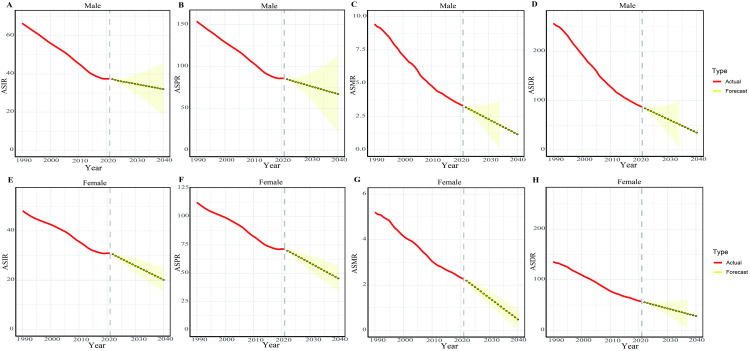
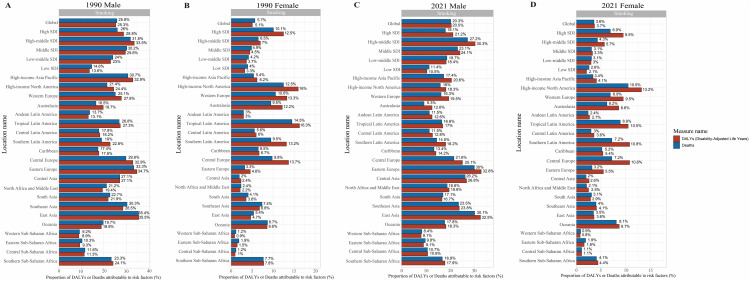
Results: The global incidence and prevalence cases of PUD increased by 11.1% and 8.8%, respectively, between 1990 and 2021. In contrast, the number of deaths and DALYs decreased by 15.94% and 27.8%, respectively, during the same period. The global age-standardized rates (ASRs) for incidence, prevalence, deaths and DALYs associated with PUD decreased by 40.3%, 41.1%, 61.5%, and 63.1%, respectively, between 1990 and 2021. Men exhibited higher numbers and ASRs of incidence, prevalence, deaths, and DALYs associated with PUD than women across most age cohorts in 2021.The average annual percentage change (AAPC) in age-standardized incidence (ASIR), prevalence (ASPR), deaths (ASMR), and DALYs (ASDR) rates for PUD were -1.65 (95% confidence interval (CI): -1.69, -1.61), -1.69 (95% CI: -1.74, -1.63), -3.02 (95% CI: -3.13, -2.91) and -3.17 (95% CI: -3.24,-3.10), respectively, from 1990 to 2021 on a global scale. In 2021, negative associations were observed globally among the ASIR, ASPR, ASMR, ASDR and the Socio-Demographic Index (SDI). Based on the ARIMA model, we projected that the global ASIR, ASPR, ASMR, and ASDR for PUD will exhibit decreasing trends from 2022 to 2040 for both sexes. We also identified smoking as the primary risk factor associated with PUD-related DALYs and deaths in both sexes in 1990 and 2021.
Conclusion: Significant advancements have been noted in reducing the global burden of PUD. Nonetheless, significant geographical and gender disparities exist in PUD numbers and ASRs, suggesting that a substantial portion of the population still lacks access to quality healthcare or experiences variations in risk factors for PUD. Thus, precise prevention strategies are essential to mitigate the disease burden of PUD.
Copyright: © 2025 Hao et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
