

Association between self-administrated prophylactics and SARS-CoV-2 infection among traditional market vendors from the Central Highlands of Peru: A nested case-control study
- PMID: 40644504
- PMCID: PMC12250348
- DOI: 10.1371/journal.pone.0327746
Association between self-administrated prophylactics and SARS-CoV-2 infection among traditional market vendors from the Central Highlands of Peru: A nested case-control study
Abstract
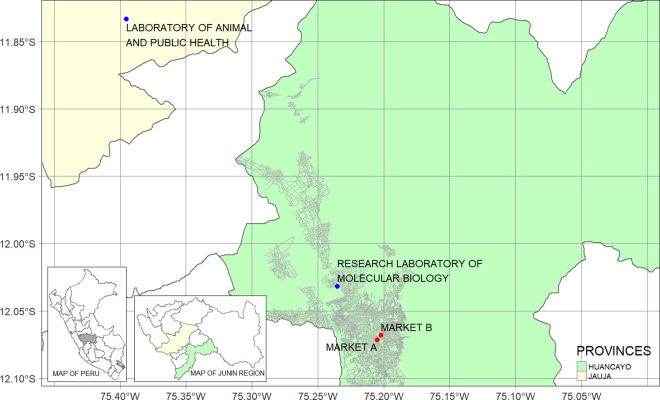
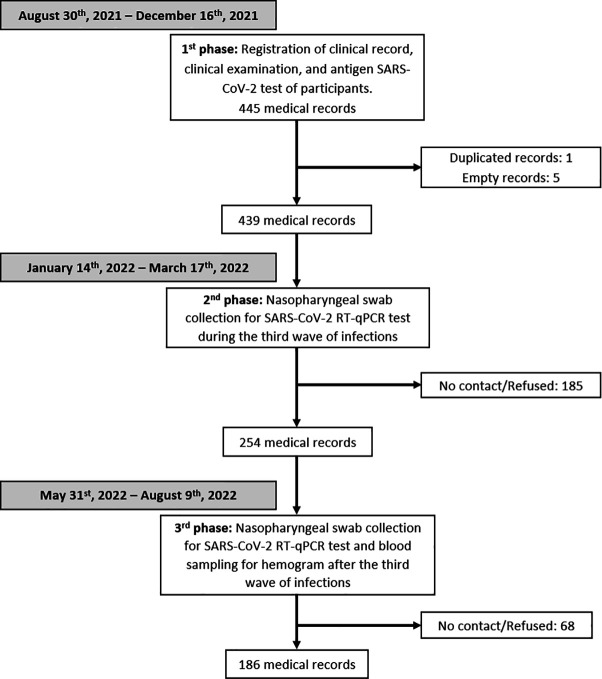
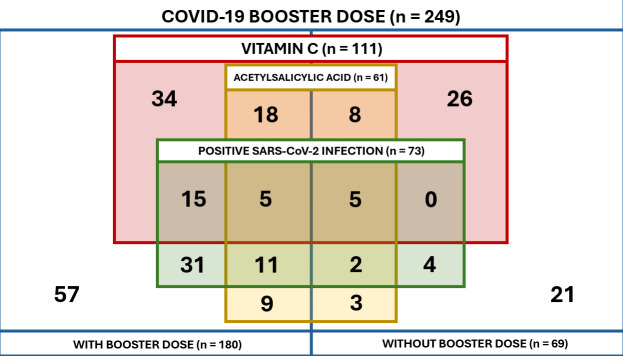
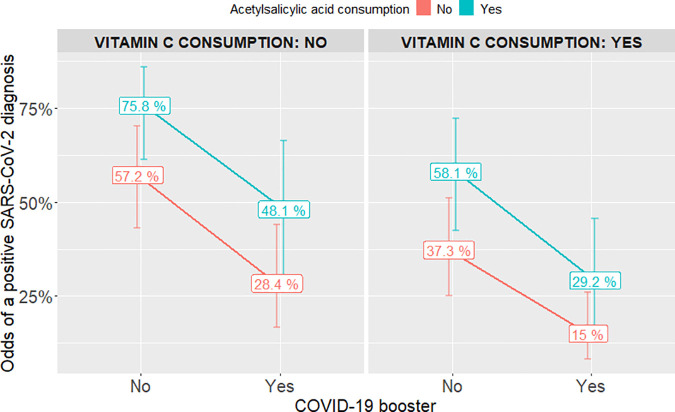
Although COVID-19 is no longer a public health emergency of international concern, understanding behaviours such as self-medication remains relevant for informing future outbreak responses and improving public health preparedness. Despite its widespread use during the pandemic, research on medications preventing SARS-CoV-2 infection in healthy individuals is scarce. We investigated the association between self-administered prophylactics and SARS-CoV-2 infection during the third wave of the pandemic in Peru. A nested case-control study was carried out in a cohort of traditional market vendors in the Peruvian Central Highlands, enrolled in a health program. Cases (positive SARS-CoV-2 diagnosis) were matched with controls (negative) by age, sex, and market of origin. Conditional logistic regression models were fitted to evaluate the association between self-administered prophylactics and SARS-CoV-2 infection. As a result, 73 cases were matched with 176 controls. Acetylsalicylic acid consumption increased SARS-CoV-2 infection odds (adjusted Odds Ratio 2.34; 95% Confidence Interval 1.17-4.66). Conversely, vitamin C consumption reduced infection odds (adjusted Odds Ratio 0.44; 95% Confidence Interval 0.23-0.87). Finally, not having the COVID-19 booster increased infection odds (adjusted Odds Ratio 3.38; 95% Confidence Interval 1.43-7.95). In conclusion, our findings suggest that acetylsalicylic acid consumption increased the odds of SARS-CoV-2 infection, whereas vitamin C consumption decreased the infection odds during the third epidemic wave in Peru. Further research on the use of these medications is needed to establish a robust causal relationship with SARS-CoV-2 infection.
Copyright: © 2025 Andrade et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Centro Nacional de Epidemiología, Prevención y Control de Enfermedades. Pacientes post-vacunas hospitalizados y estado vacunal. In: Tablero de hospitalizados y vacunas. Accessed 2023 December 3 https://www.dge.gob.pe/dashhospitalizadosvacunas/#grafico04
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
