

The morphological spectrum of Castleman disease and related disorders: a report from the Lymphoma Workshop of the 22nd Meeting of the European Association of Hematopathology
- PMID: 40646240
- PMCID: PMC12391218
- DOI: 10.1007/s00428-025-04171-w
The morphological spectrum of Castleman disease and related disorders: a report from the Lymphoma Workshop of the 22nd Meeting of the European Association of Hematopathology
Abstract
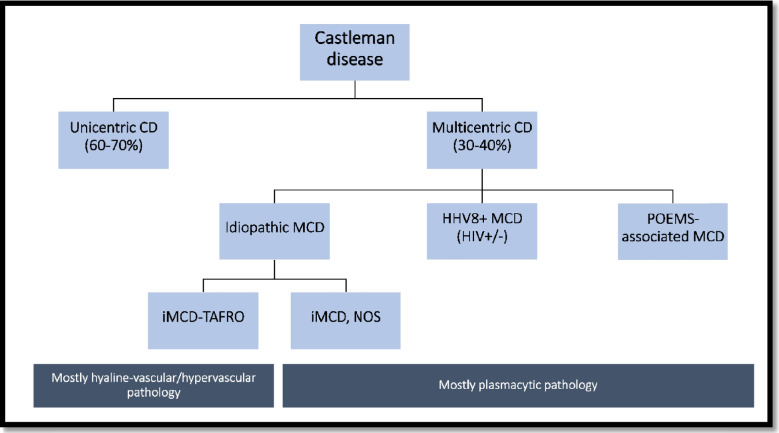
Castleman disease (CD) is an intriguing and complicated group of local and systemic disorders mainly affecting lymph nodes with heterogeneous presentation and therapeutic needs. These disorders were the topic of Session 1 of the Lymphoma Workshop at the 2024 EA4HP in Dubrovnik, Croatia. In this report, we summarize the features of the 85 submitted cases and review the differential diagnosis, pitfalls, and advances for all CD subtypes. Specifically, the molecular landscape of unicentric CD and its relationship with follicular dendritic cell proliferations and indolent T-lymphoblastic proliferation will be discussed. The spectrum of idiopathic multicentric CD (MCD), TAFRO syndrome, as well as the clinical and histopathological peculiarities of POEMS-CD, is reviewed. Cases of Kaposi sarcoma-associated herpesvirus/human herpesvirus 8 (KSHV/HHV8) + MCD were the most complicated and well demonstrated the difficulties and overlaps in the differential diagnosis of KSHV/HHV8 + lymphoproliferative disorders. Finally, the important topic of CD mimickers will be addressed, demonstrating how the integration of clinical, laboratory, histopathological, and molecular data is mandatory to confirm a diagnosis of CD and how to distinguish it from the many neoplastic, autoimmune, and infective mimickers.
Keywords: CD-mimickers; Castleman disease; Idiopathic multicentric Castleman disease; KSHV/HHV8-associated lymphoproliferative disorders; POEMS syndrome; TAFRO syndrome.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors declare no competing interests.
Figures


References
-
- Weisenburger DD (Mar.1988) Multicentric angiofollicular lymph node hyperplasia. Pathology of the spleen. Am J Surg Pathol 12(3):176–181. 10.1097/00000478-198803000-00002 - PubMed
-
- Wang L et al (Aug.2020) Predominant stroma-rich feature in hyaline vascular variant of castleman disease is associated with paraneoplastic pemphigus. Am J Clin Pathol 154(3):403–413. 10.1093/ajcp/aqaa053 - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
