

Prophylactic mesh reinforcement in elective abdominal surgeries: a systematic review, meta-analysis, and GRADE evidence assessment
- PMID: 40646274
- PMCID: PMC12254175
- DOI: 10.1007/s10029-025-03421-9
Prophylactic mesh reinforcement in elective abdominal surgeries: a systematic review, meta-analysis, and GRADE evidence assessment
Abstract
Background: Elective laparotomies account for a larger fraction of laparotomy procedures performed worldwide. Although surgical techniques continue to advance, the incidence of incisional hernia (IH) and other post-operative complications remain challenging to surgeons. This study aimed to evaluate the significance of using prophylactic mesh reinforcement during elective laparotomy.
Methods: A comprehensive search was conducted in PubMed, Scopus, and Web of Science to identify studies that included adults undergoing elective abdominal surgery and compared prophylactic mesh reinforcement of the abdominal wall using any type of mesh in any anatomical position to standard fascial closure with sutures alone, without mesh. The analysis aimed to assess the impact of mesh reinforcement on the incidence of IH at all possible timepoints, in addition to secondary outcomes based on mesh technique, such as wound infections, dehiscence, seroma, re-operation for IH, and prolonged hospital stay. Data analysis was performed using the R programming language.
Results: Fifteen RCTs, including 2,233 patients with follow-up durations ranging from 1.5 to 5 years, were analyzed. Prophylactic mesh reinforcement significantly reduced the incidence of IH following elective gastrointestinal surgeries at 12 months (risk ratio [RR] = 0.35, 95% confidence interval [CI] [0.14; 0.86], p = 0.02), 24 months (RR = 0.28, 95% CI [0.11; 0.68], p < 0.01), 36 months (RR = 0.62, 95% CI [0.36; 1.06], p = 0.08), and 48 months (RR = 0.35, 95% CI [0.11; 1.17], p = 0.09). Similarly, mesh significantly reduced IH rates following open abdominal aortic aneurysm repair at 12 months (RR = 0.13, 95% CI [0.04; 0.41], p < 0.01), 24 months (RR = 0.31, 95% CI [0.21; 0.45], p < 0.01), and 36 months (RR = 0.23, 95% CI [0.10; 0.54], p < 0.01).
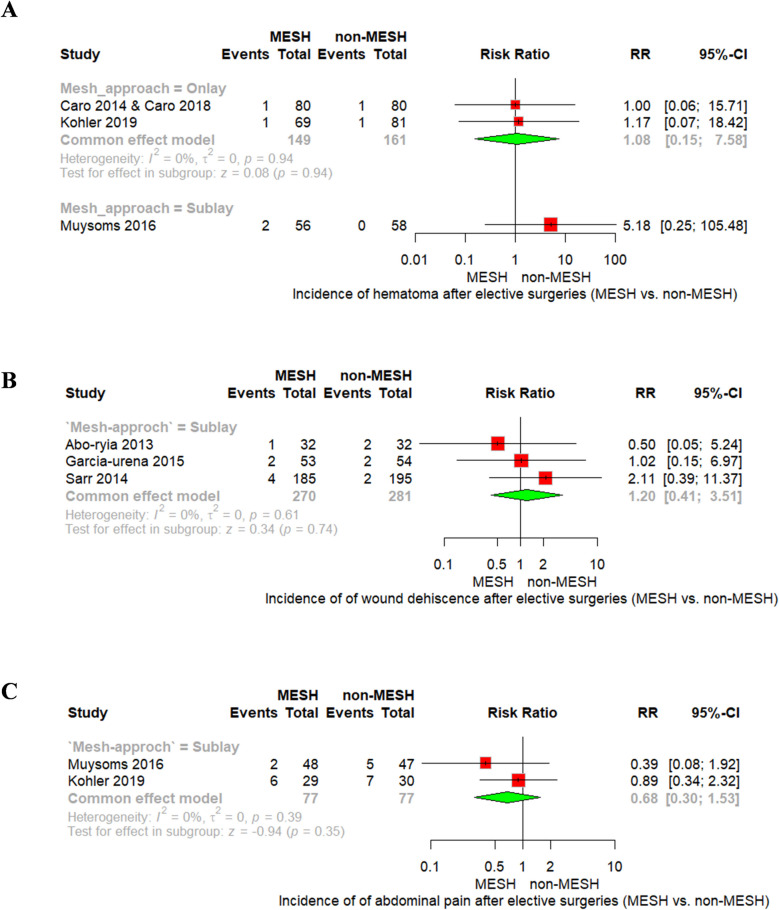
Conclusions: Prophylactic mesh reinforcement during elective abdominal laparotomy significantly reduced the incidence of IH and the need for reoperation. However, it is associated with an increased risk of seroma formation and, to a lesser extent, wound infection, particularly with the Sublay technique.
Keywords: Abdominal wall closure; Elective laparotomy; Incisional hernia; MESH.
© 2025. The Author(s).
Conflict of interest statement
Declarations. All authors have shared in the final drafting of the manuscript. All authors have read and approved the final manuscript. Ethics approval and consent to participate: This article does not contain any studies with human participants or animals performed by any of the authors. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests. Submission declaration: We confirm that this manuscript has not been published elsewhere and is not under consideration by another journal. All authors have approved the manuscript and agree with its submission to Hernia.
Figures






References
-
- Nachiappan S, Markar S, Karthikesaligam A, Ziprin P, Faiz O (2013) Prophylactic mesh placement in high-risk patients undergoing elective laparotomy: a systematic review. World J Surg 37:1861–1871. 10.1007/s00268-013-2046-1 - PubMed
-
- Kingsnorth A, LeBlanc K (2003) Hernias: inguinal and incisional. Lancet 362:1561–1571. 10.1016/S0140-6736(03)14746-0 - PubMed
-
- Sanders DL, Kingsnorth AN (2012) The modern management of incisional hernias. BMJ 344:e2843–e2843. 10.1136/bmj.e2843 - PubMed
-
- Burger JWA, Van’T Riet M, Jeekel J (2002) Abdominal incisions: Techniques and postoperative complications. Scand J Surg 91:315–321. 10.1177/145749690209100401 - PubMed
-
- Wissing J, Van Vroonhoven TJMV, Schattenkerk ME, Veen HF, Ponsen RJG, Jeekel J (1987) Fascia closure after midline laparotomy: Results of a randomized trial. J Br Surg 74:738–741. 10.1002/bjs.1800740831 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
