

Recurrent waning of anti-SARS-CoV-2 neutralizing antibodies despite multiple antigen encounters
- PMID: 40646552
- PMCID: PMC12247477
- DOI: 10.1186/s12967-025-06837-0
Recurrent waning of anti-SARS-CoV-2 neutralizing antibodies despite multiple antigen encounters
Abstract
Background: SARS-CoV-2 neutralizing antibodies may protect against symptomatic infection in immunized individuals. However, vaccine-induced antibody levels wane over time, reducing vaccine efficacy. The definition of the waning kinetics of neutralizing SARS-CoV-2 responses and the potential impact of sequential antigen encounters are still poorly defined.
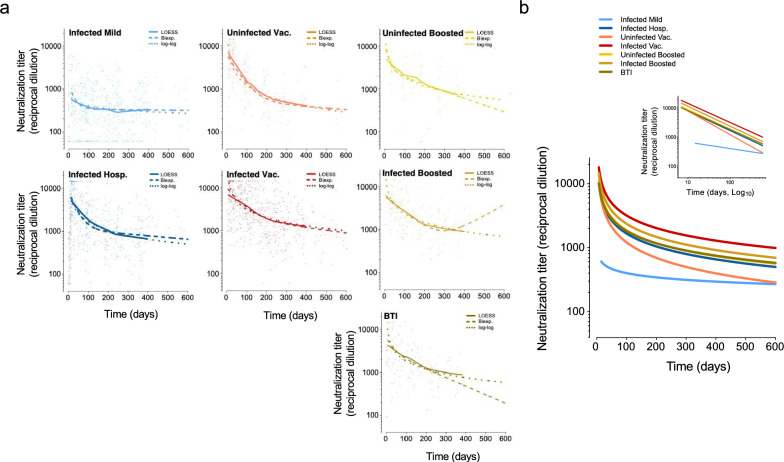
Methods: Plasma neutralizing activity was determined in longitudinally collected samples from SARS-CoV-2 infected, primo-vaccinated and boosted individuals. Neutralizing activity decay kinetics were modeled against time using Log-Log and biexponential models.
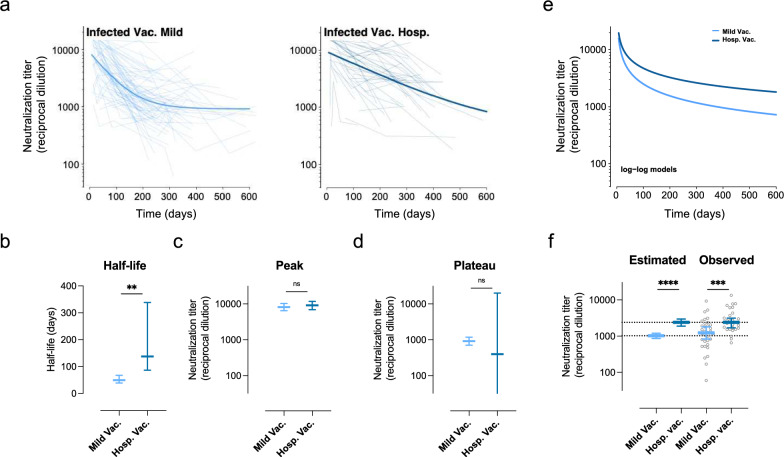
Results: Neutralizing antibody levels wane after an initial peak in all groups of vaccinated individuals with half-life ranging from 29 to 60 days. Exponential models showed a subsequent stabilization of neutralizing titers to a plateau. Both the peak response and the plateau values depended on vaccine type, infection status and severity of infection. Booster immunization by either vaccines or breakthrough infections did not modify peak, plateau or decay rate values.
Conclusions: Our results indicate that the waning of SARS-CoV-2 neutralizing antibody responses was recurrent even after several antigen encounters. Repeated immunizations would be required to maintain high levels of neutralizing antibodies and protect vulnerable individuals from symptomatic infection.
Keywords: Booster; Breakthrough infection; COVID-19; Humoral response; Hybrid immunity; Kinetics; Neutralization; Vaccine.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The studies were approved by the Hospital Ethics Committee Board from Hospital Universitari Germans Trias i Pujol (HUGTiP: PI-20-122, PI-20-217 and PI-21-351 for KING, KING cohort extension and KING-VAX cohorts, respectively). All participants provided written informed consent. Consent for publication: Not applicable. Competing interests: J.B. declares institutional grants from HIPRA, NESAPOR EUROPE and MSD, and personal consultancy fees from NESAPOR EUROPE and HIPRA. Unrelated to the submitted work, J.B. and J.C. were founders and shareholders of AlbaJuna Therapeutics. SL. B.C. was founder and shareholder of AlbaJuna Therapeutics SL. and AELIX Therapeutics. SL. The other authors declare no competing interests.
Figures




References
-
- Sette A, Sidney J, Crotty S. T cell responses to SARS-CoV-2. Annu Rev Immunol. 2023;41:343–73. - PubMed
-
- Khoury DS, Cromer D, Reynaldi A, Schlub TE, Wheatley AK, Juno JA, et al. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat Med. 2021;27:1205–11. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
