

Cerebral small vessel disease in memory center patients with dementia with lewy bodies and Alzheimer's disease
- PMID: 40646592
- PMCID: PMC12254957
- DOI: 10.1186/s13195-025-01805-8
Cerebral small vessel disease in memory center patients with dementia with lewy bodies and Alzheimer's disease
Abstract
Introduction: Cerebral small vessel disease (CSVD) is a common co-pathology in patients with dementia with Lewy bodies (DLB) and Alzheimer's disease (AD). A comprehensive characterization of CSVD load in DLB and AD patients referred to a memory center is lacking.
Methods: In this retrospective study, we collected data from patients with a clinical DLB diagnosis or clinico-biological AD diagnosis, evaluated at our memory center. They were assessed for CSVD MRI features, including enlarged perivascular spaces (PVS), presence of cerebral amyloid angiopathy (CAA) and hypertensive arteriopathy (HTNA). Differences in CSVD features between AD and DLB and across clinical stages were investigated. Regression models were used to evaluate the association between (i) cerebrovascular risk factors (CVRF) and HTNA, and (ii) CSVD features and cognition as expressed by Montreal Cognitive Assessment (MoCA).
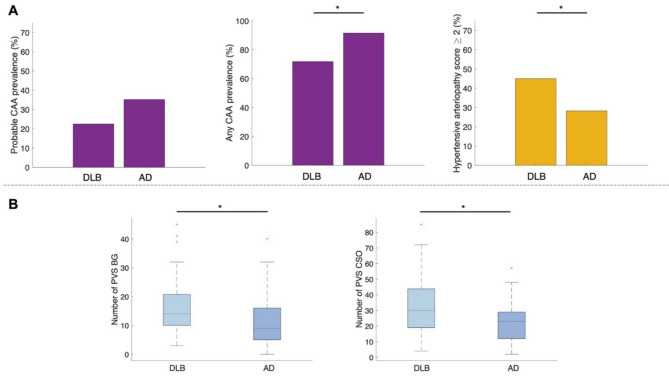
Results: We included 71 DLB (76.8 ± 7.4 years old, 25 females) and 71 age- and sex-matched AD patients (and 75.2 ± 5.3 years old, 27 females). Probable CAA, according to current Boston 2.0 criteria, was observed in 22.5% of DLB and 35.2% of AD patients, while any (probable + possible) CAA rate was higher in the two groups (71.8% and 91.5%, respectively). A moderate/severe HTNA was present in 45% of DLB and 28.2% of AD patients. When comparing the two groups, DLB presented with higher HTNA score (p =.012), while AD patients had higher prevalence of any CAA (p =.002). Patients with DLB had a greater PVS burden in the basal ganglia (p =.011) and centrum semiovale (p =.004) and higher number of deep microbleeds (p =.004). Certain HTNA-related features were more pronounced at dementia stage, with respect to mild cognitive impairment. No association was observed between CVRF and HTNA. Regarding the association between CSVD and cognition, only deep microbleeds count was related to MoCA in DLB patients.
Discussion: DLB or AD patients present with high CSVD burden and differ in terms of features and subtype. Patients with DLB present with increased HTNA, PVS load and deep microbleeds, while patients with AD present with a higher any CAA prevalence. CSVD might impact global cognition.
Keywords: AD; Alzheimer’s disease; CSVD; Cerebral small vessel disease; DLB; Dementia with lewy bodies; Perivascular spaces.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: G. Bommarito: reports no disclosures relevant to the manuscript. A. Griffa: reports no disclosures relevant to the manuscript. P. Michel: reports no disclosures relevant to the manuscript. C. Hall: reports no disclosures relevant to the manuscript. P. Salvioni-Chiabotti: reports no disclosures relevant to the manuscript. S. Pistocchi: reports no disclosures relevant to the manuscript. Y. Aleman-Gomez: reports no disclosures relevant to the manuscript. D. Damian: reports no disclosures relevant to the manuscript. M. Jreige: reports no disclosures relevant to the manuscript. J. O. Prior: reports no disclosures relevant to the manuscript. V. Dunet: reports no disclosures relevant to the manuscript. O. Rouaud: reports no disclosures relevant to the manuscript. P. Hagmann: reports no disclosures relevant to the manuscript. G. Allali reports no disclosures relevant to the manuscript.
Figures
Similar articles
-
Prevalence, distribution, and severity of cerebral amyloid angiopathy differ between Lewy body diseases and Alzheimer's disease.Acta Neuropathol Commun. 2024 Feb 15;12(1):28. doi: 10.1186/s40478-023-01714-7. Acta Neuropathol Commun. 2024. PMID: 38360761 Free PMC article.
-
Dopamine transporter imaging for the diagnosis of dementia with Lewy bodies.Cochrane Database Syst Rev. 2015 Jan 30;1(1):CD010633. doi: 10.1002/14651858.CD010633.pub2. Cochrane Database Syst Rev. 2015. PMID: 25632881 Free PMC article.
-
Relationship between cerebral small vessel disease and proteinopathies in the medial temporal lobe.Acta Neuropathol Commun. 2025 Jul 16;13(1):156. doi: 10.1186/s40478-025-02076-y. Acta Neuropathol Commun. 2025. PMID: 40671047 Free PMC article.
-
Cerebral amyloid angiopathy in patients with Dementia with Lewy Bodies: A clinical and hippocampal morphology study.Parkinsonism Relat Disord. 2025 Aug;137:107892. doi: 10.1016/j.parkreldis.2025.107892. Epub 2025 May 26. Parkinsonism Relat Disord. 2025. PMID: 40479839
-
CSF tau and the CSF tau/ABeta ratio for the diagnosis of Alzheimer's disease dementia and other dementias in people with mild cognitive impairment (MCI).Cochrane Database Syst Rev. 2017 Mar 22;3(3):CD010803. doi: 10.1002/14651858.CD010803.pub2. Cochrane Database Syst Rev. 2017. PMID: 28328043 Free PMC article.
References
-
- Niedowicz DM, Nelson PT, Murphy MP. Alzheimers Disease: Pathological Mechanisms and Recent Insights [Internet]. Curr. Neuropharmacol. 2011. pp. 674–84. Available from: http://www.eurekaselect.com/article/20860 - PMC - PubMed
-
- Arvanitakis Z, Capuano AW, Leurgans SE, Bennett DA, Schneider JA. Relation of cerebral vessel disease to Alzheimer’s disease dementia and cognitive function in elderly people: a cross-sectional study. Lancet Neurol [Internet]. 2016;15:934–43. Available from: 10.1016/S1474-4422(16)30029-1 - PMC - PubMed
-
- Jellinger KA. Significance of cerebral amyloid angiopathy and other co-morbidities in lewy body diseases. J Neural Transm. 2021;128:687–99. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
