

Antiplatelet Therapy Mitigates Brain Metastasis Risk in Non-Small Cell Lung Cancer: Insights from a Comprehensive Retrospective Study
- PMID: 40647360
- PMCID: PMC12248695
- DOI: 10.3390/cancers17132059
Antiplatelet Therapy Mitigates Brain Metastasis Risk in Non-Small Cell Lung Cancer: Insights from a Comprehensive Retrospective Study
Abstract
Background: Brain metastases are a common and devastating complication of non-small cell lung cancer (NSCLC), severely affecting prognosis and quality of life. Despite increasing interest in the role of platelets in tumor progression and dissemination, the potential impact of antiplatelet therapy on brain metastasis in NSCLC remains underexplored.
Methods: In this retrospective observational study, we analyzed data from 650 patients diagnosed with NSCLC over a four-year period to evaluate whether prior or subsequent exposure to antiplatelet agents correlates with a reduced incidence of brain metastases.
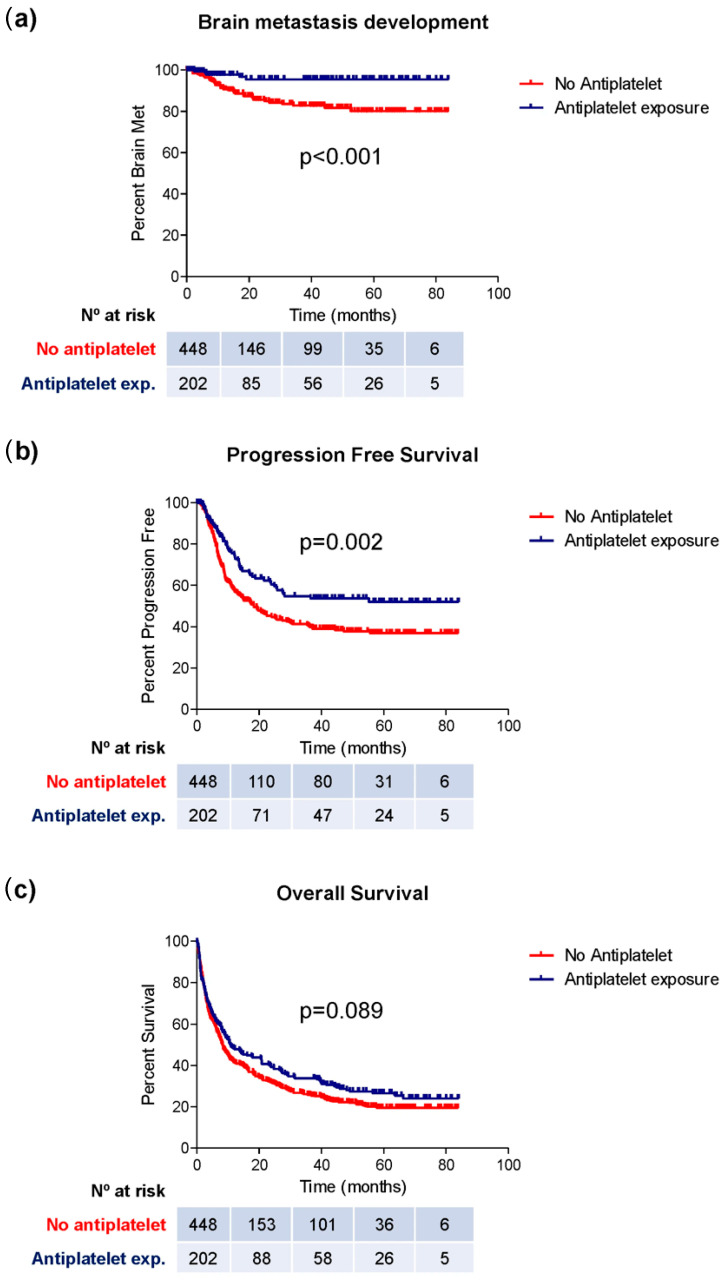
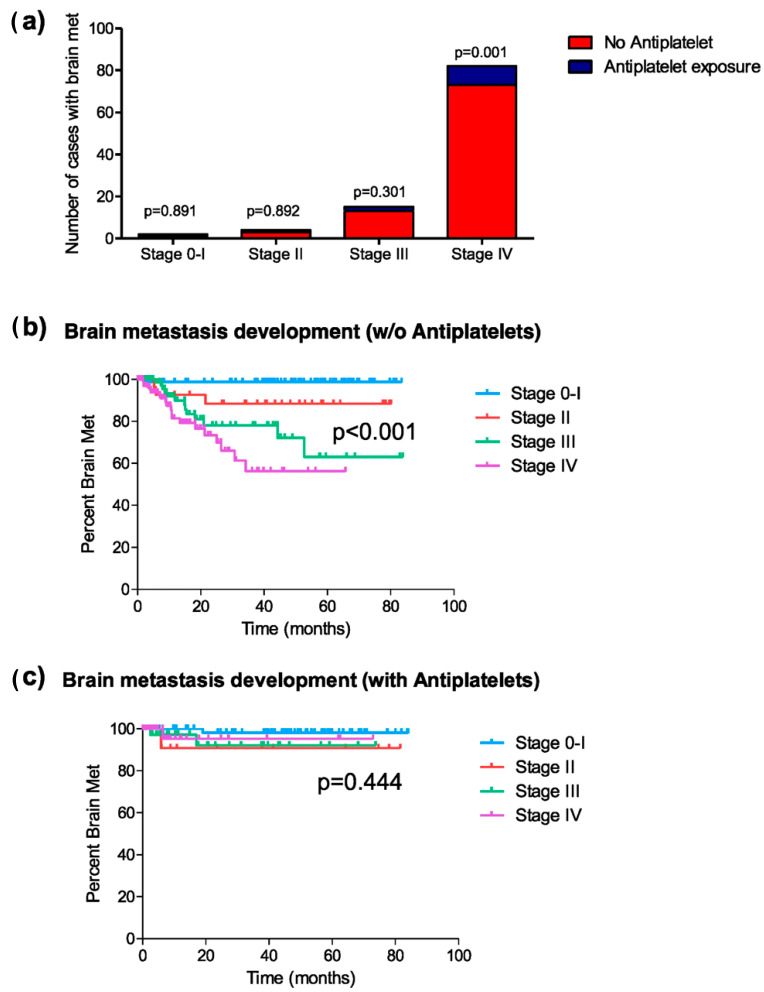
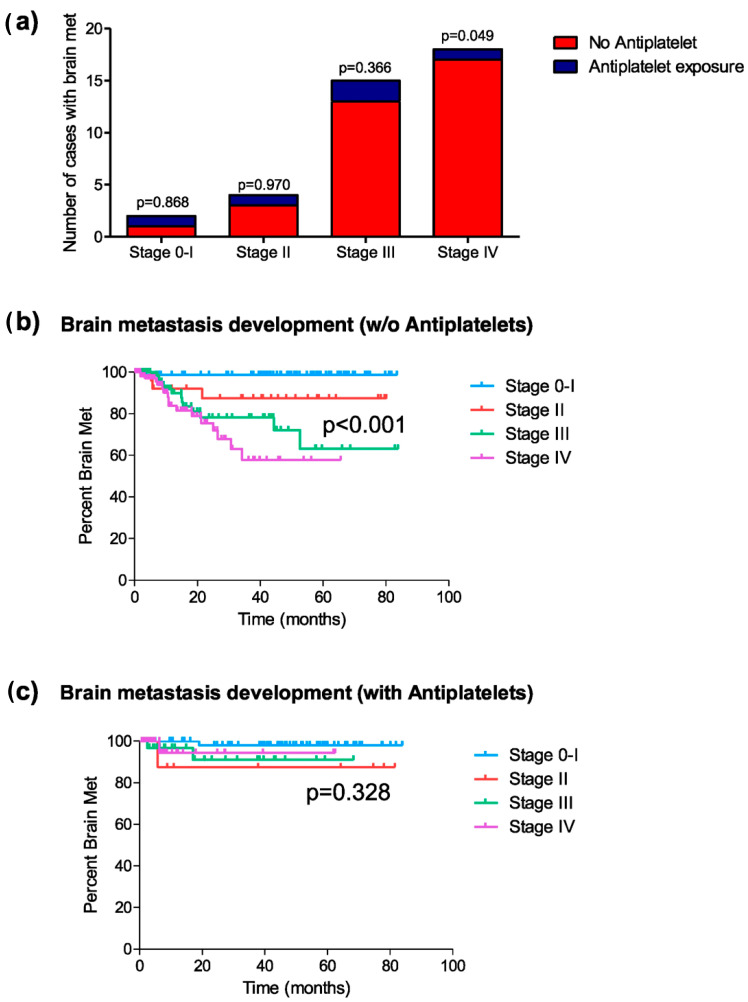
Results: Patients exposed to antiplatelet therapy, predominantly aspirin, presented with more comorbidities and were generally older. Despite these differences, they showed a significantly lower risk of developing brain metastases during the disease course (6.9% vs. 20.0%, p < 0.001), particularly among those with advanced-stage disease at diagnosis. A longer time to metastasis development was also observed in antiplatelet users (77.5 vs. 62.6 months, p < 0.001), along with improved progression-free survival. Additionally, patients on antiplatelets before diagnosis had a lower probability of presenting brain metastases at the time of diagnosis (3.9% vs. 12.1%, p = 0.014), and no cases of brain metastases occurred in patients who started antiplatelet therapy shortly after diagnosis. These findings highlight the potential of antiplatelet agents to interfere with key mechanisms of metastatic spread, including immune evasion and premetastatic niche formation.
Conclusions: Importantly, this study provides one of the first real-world analyses suggesting a consistent and stage-dependent association between antiplatelet use and reduced brain metastatic burden in NSCLC. By bridging the gap between preclinical insights and clinical outcomes, our work offers a novel and clinically relevant perspective that supports further research into the integration of antiplatelet therapy in NSCLC management.
Keywords: antiplatelet therapy; brain metastases; non-small cell lung cancer (NSCLC); platelet–tumor interaction; real-world evidence.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Planchard D., Popat S., Kerr K., Novello S., Smit E.F., Faivre-Finn C., Mok T.S., Reck M., Van Schil P.E., Hellmann M.D., et al. Metastatic Non-Small Cell Lung Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2018;29:iv192–iv237. doi: 10.1093/annonc/mdy275. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
