

Review
doi: 10.3390/cancers17132074.
Beyond the Signal: Imaging Insights and Diagnostic Relevance of Bone Oedema in Bone Tumours and Tumour-like Lesions
Affiliations
- PMID: 40647375
- PMCID: PMC12248669
- DOI: 10.3390/cancers17132074
Item in Clipboard
Review
Beyond the Signal: Imaging Insights and Diagnostic Relevance of Bone Oedema in Bone Tumours and Tumour-like Lesions
Cancers (Basel).
.
Abstract
Bone oedema is a non-specific imaging finding associated with a wide range of pathologies, including trauma, infection, inflammation, and neoplasms [...].
Keywords: MRI; Oedema; bone; bone tumour; magnetic resonance imaging.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

T1-weighted (A) and STIR (B) sagittal MRI demonstrating a chondroblastoma of the anterior calcaneus, with florid perilesional intramedullary oedema, greater in volume than the lesion itself.

Lower leg axial CT image (A), axial T1-weighted (B), and STIR (C) axial MRI demonstrate the cortical thickening and extensive adjacent periosteal and soft tissue oedema.

Coronal CT (A) and STIR MRI (B) demonstrating an osteoblastoma of the medial cuneiform, with marked surrounding sclerosis and both osseous and soft tissue oedema, larger than the size of the lesion itself. Sagittal T1-weighted (C) and STIR (D) coronal MRI demonstrate the oedema involving almost the entire medial cuneiform.

Anteroposterior radiograph (A) and coronal T1-weighted (B) and STIR (C) MRI showing Langerhans cell histiocytosis of the proximal humeral metadiaphysis, characterised by a permeative pattern of lysis and florid oedema throughout the affected medulla and adjacent soft tissues.

T1 (A) and STIR (B) coronal MRI images demonstrating stress fracture of the proximal fibula with intramedullary, periosteal and extraosseous oedema, along with a low signal fracture line.

Humeral anteroposterior radiograph (A), sagittal T1-weighted (B) and STIR (C) MRI, demonstrating large intraosseous abscesses with the penumbra sign and marked surrounding intramedullary oedema, with free fat globules present, more so at the proximal metaphysis.

Dorsoplantar radiograph (A) and STIR sagittal MRI (B) demonstrating florid reactive periostitis and extensive local osseous and soft tissue oedema. Subsequent radiograph (C) demonstrates consolidation of the periostitis ossificans.

Shoulder anteroposterior radiograph (A), T1-weighted (B), and STIR coronal MRI (C) demonstrating calcific tendinitis of the supraspinatus tendon (arrowhead), with intraosseous migration (white arrow) and florid intramedullary oedema.

Sagittal (A) and coronal (B) STIR MRI demonstrating florid osseous oedema of the cuboid, secondary to peroneus longus tendinopathy.

T1-weighted (A) and STIR (B) sagittal MRI demonstrating tophi at the distal quadriceps and proximal patellar tendons, with only mild oedema in the adjacent bone.

Anteroposterior radiograph (A) and T1-weighted (B) and STIR (C) MRI of a distal femoral osteosarcoma, demonstrating an aggressive periosteal reaction in the form of a Codman triangle, and a large soft tissue component. The volume of osseous oedema is less than that of the tumour itself. A macroscopic resection specimen of a different osteosarcoma is also shown (D).

Sagittal CT reconstruction (A), coronal T1-weighted (B) and T2-weighted (C) MRI demonstrate a large soft tissue mass projected over the proximal medial thigh with internal calcification and no significant associated osseous or extraosseous oedema. Macroscopic resection specimen (D) of a proximal femoral chondrosarcoma, complicated by pathological fracture.
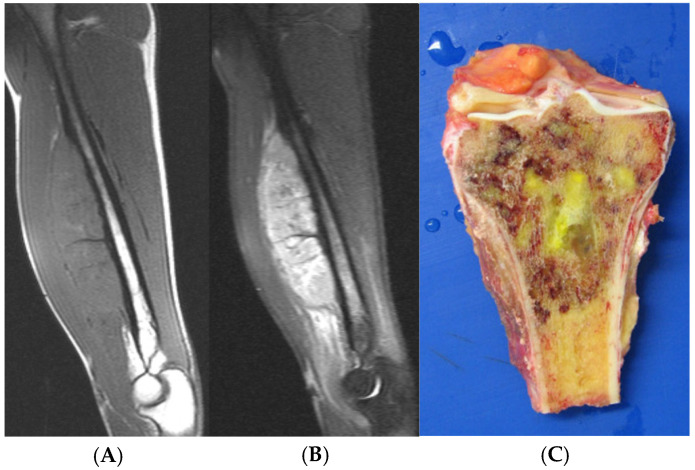
Sagittal T1-weighted (A) and STIR (B) MRI of a Ewing’s sarcoma of the humerus. Note the soft tissue component which is larger than the volume of the osseous oedema. Macroscopic resection specimen (C) of a proximal tibial Ewing’s sarcoma.
Similar articles
-
Histopathological perspective on bone marrow oedema, reactive bone change and haemorrhage.Eur J Radiol. 2008 Jul;67(1):62-7. doi: 10.1016/j.ejrad.2008.01.056. Epub 2008 Mar 12. Eur J Radiol. 2008. PMID: 18337044
-
Computed tomography versus magnetic resonance imaging versus bone scintigraphy for clinically suspected scaphoid fractures in patients with negative plain radiographs.Cochrane Database Syst Rev. 2015 Jun 5;2015(6):CD010023. doi: 10.1002/14651858.CD010023.pub2. Cochrane Database Syst Rev. 2015. PMID: 26045406 Free PMC article.
-
Computed tomography and/or magnetic resonance imaging for pre-operative planning for inverted nasal papilloma: review of evidence.J Laryngol Otol. 2009 Jul;123(7):705-9. doi: 10.1017/S0022215109004575. Epub 2009 Feb 16. J Laryngol Otol. 2009. PMID: 19216815
-
Magnetic resonance perfusion for differentiating low-grade from high-grade gliomas at first presentation.Cochrane Database Syst Rev. 2018 Jan 22;1(1):CD011551. doi: 10.1002/14651858.CD011551.pub2. Cochrane Database Syst Rev. 2018. PMID: 29357120 Free PMC article.
-
¹⁸F-FDG PET/CT: a review of diagnostic and prognostic features in multiple myeloma and related disorders.Clin Exp Med. 2015 Feb;15(1):1-18. doi: 10.1007/s10238-014-0308-3. Epub 2014 Sep 14. Clin Exp Med. 2015. PMID: 25218739
References
Publication types
LinkOut - more resources
Full Text Sources
