

Hydrocodone Rescheduling and Opioid Prescribing Disparities in Breast Cancer Patients
- PMID: 40647445
- PMCID: PMC12248469
- DOI: 10.3390/cancers17132146
Hydrocodone Rescheduling and Opioid Prescribing Disparities in Breast Cancer Patients
Abstract
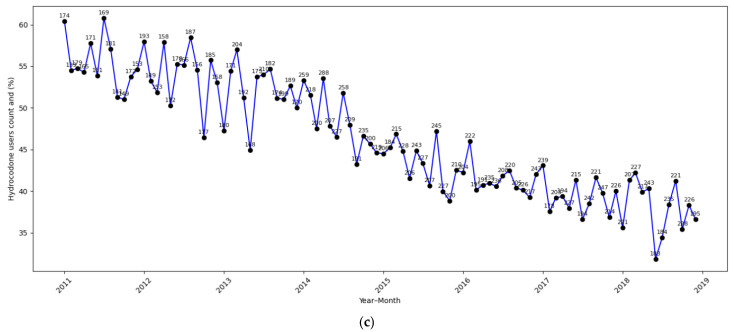
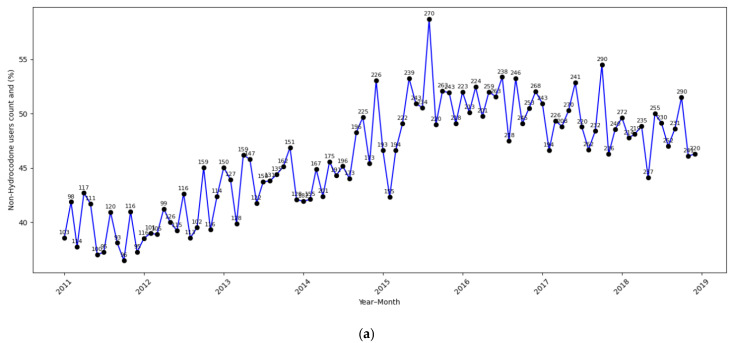
Background: Pain is a prevalent issue among breast cancer patients and survivors, with a significant proportion receiving hydrocodone for pain management. However, the rescheduling of hydrocodone from Schedule III to Schedule II by the U.S. Drug Enforcement Administration (DEA) in October 2014 raised concerns about potential barriers to opioid access for cancer patients, particularly among vulnerable populations such as dually eligible Medicare-Medicaid beneficiaries and racial/ethnic minorities. Methods: We conducted a retrospective cohort study using Surveillance, Epidemiology, and End Results (SEER)-Medicare linked data including 52,306 early-stage breast cancer patients from 2011 to 2019. We employed multivariable logistic regression models with model specification tests to stratify the subgroups and evaluate the differential effects of the policy change by Medicaid dual eligibility and race-ethnicity, while adjusting for other patient demographics, clinical characteristics, and cancer treatments. Results: The rescheduling of hydrocodone was associated with significantly different effects on prescription opioid use across subgroups, with the most pronounced reduction in hydrocodone prescription observed among dual-eligible racial/ethnic minority patients (adjusted odds ratio [AOR] = 0.57; 95% confidence interval [CI]: 0.44-0.74; p < 0.001). Non-dual-eligible patients experienced a smaller reduction in hydrocodone use (AOR = 0.84; 95% CI: 0.78-0.90; p < 0.001). Concurrently, non-hydrocodone opioid use significantly increased among non-dual-eligible non-Hispanic White patients (AOR = 1.29; 95% CI: 1.19-1.40; p < 0.001), suggesting a substitution effect, while smaller non-significant increases were observed among other subgroups. Conclusions: Hydrocodone rescheduling led to the greatest reduction in hydrocodone use among dual-eligible racial-ethnic minority patients. The corresponding increase in non-hydrocodone opioid use was limited to non-dual-eligible non-Hispanic White patients. These findings highlight the need for opioid policies that balance misuse prevention with equitable access to pain relief, particularly among underserved populations.
Keywords: Medicaid; Medicare; SEER; breast cancer; hydrocodone rescheduling; opioids; pain management; race–ethnicity.
Conflict of interest statement
The authors have no conflicts of interest to declare in relation to this study.
Figures


References
-
- International Narcotics Control Board . Comments on the Reported Statistics on Narcotic Drugs. International Narcotics Control Board; Vienna, Austria: 2018.
Grants and funding
LinkOut - more resources
Full Text Sources
