

A Histopathological and Surgical Analysis of Gastric Cancer: A Two-Year Experience in a Single Center
- PMID: 40647518
- PMCID: PMC12248514
- DOI: 10.3390/cancers17132219
A Histopathological and Surgical Analysis of Gastric Cancer: A Two-Year Experience in a Single Center
Abstract
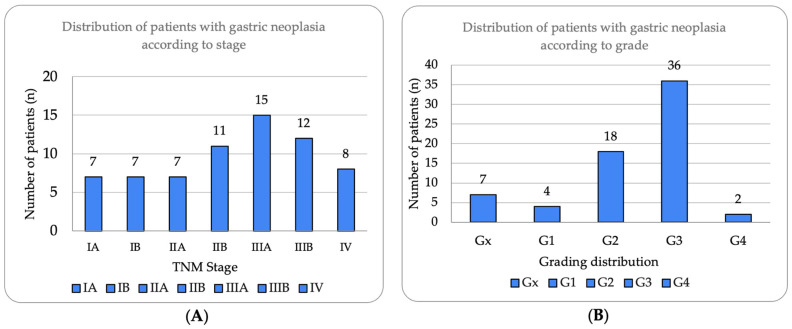
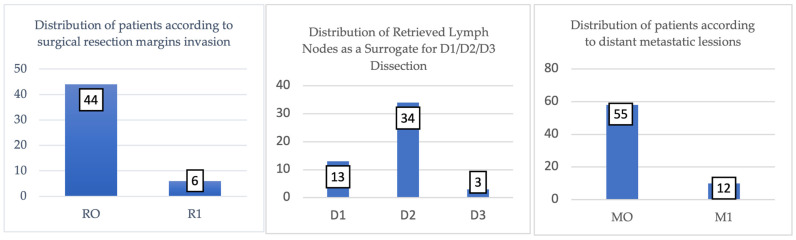
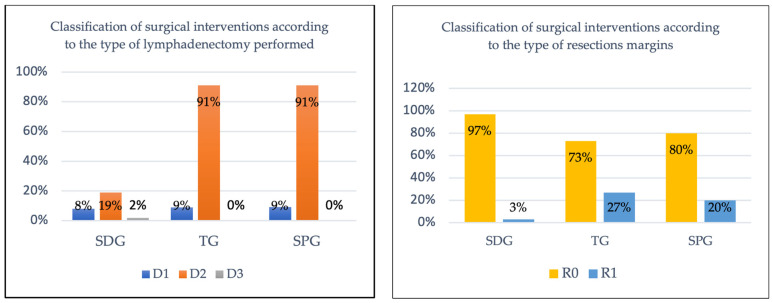
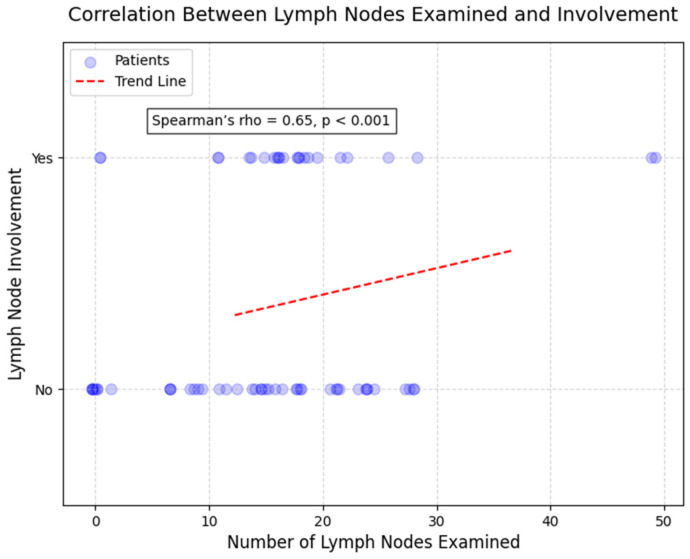
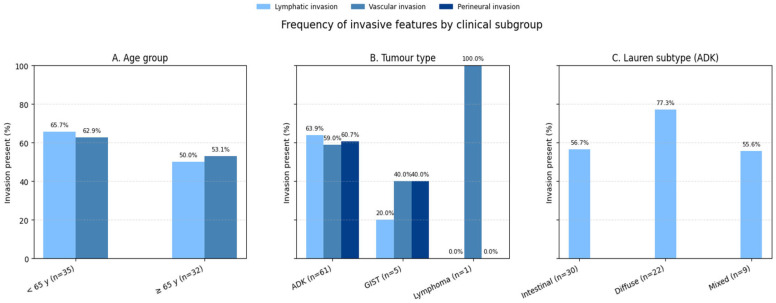
Background: Gastric neoplasms remain pathologies of the malignant spectrum with high incidence and prevalence, with their management requiring a precise histopathological characterization for optimal treatment planning. Methods: The present study is a retrospective analysis that included 67 histopathologically confirmed gastric neoplasia subjects and was performed at a single surgical center from January 2020 to December 2021. Demographics, tumor characteristics, surgical procedures, and oncologic outcomes were included, filtered, and subsequently analyzed using SPSS Statistics 29.0. Results: This study involved 67 patients (mean age 65.7 years, 56.7% men), with adenocarcinoma being the most common histologic type (91.0%) and most tumors being diagnosed directly as Stage III (40.3%). Lauren classification revealed the intestinal type as the most common (49.2%), followed by diffuse (36.1%) and mixed (14.8%). Poorly differentiated tumors (G3) accounted for 53.7% of cases. The surgical team performed curative resection in 75% (n = 50) of patients, achieving R0 margins in 88% of these cases. Subtotal gastrectomy with D2 lymphadenectomy yielded the highest curative success rate with 96.6% R0 resection. Statistically, we identified two significant correlations between age and tumor grade (rho = 0.28; p = 0.021) and between the number of lymph nodes examined and the number of lymph nodes invaded (rho = 0.65, p < 0.001). This study again revealed that adenocarcinomas showed higher rates of lymph node invasion than other tumor types (p = 0.017). Conclusions: The analysis of patients with gastric neoplasms is vital for appropriate therapeutic management. Even though the study period included a pandemic, the analysis remained a complex one with high-quality surgical outcomes, confirming the importance of maintaining oncologic standards during medical crises.
Keywords: COVID-19; Lauren classification; WHO classification; curability parameters; gastric neoplasia; histopathological characteristics; morphopathological analysis; pandemic.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Norton E.J., Bateman A.C. Intestinal Type Adenocarcinoma. PathologyOutlines.com Website. [(accessed on 25 April 2025)]. Available online: https://www.pathologyoutlines.com/topic/stomachintestinal.html.
LinkOut - more resources
Full Text Sources
