

Splenectomy in Onco-Hematologic Patients: A Retrospective Study of Early Complications and 1-Year Mortality
- PMID: 40647538
- PMCID: PMC12248626
- DOI: 10.3390/cancers17132241
Splenectomy in Onco-Hematologic Patients: A Retrospective Study of Early Complications and 1-Year Mortality
Abstract
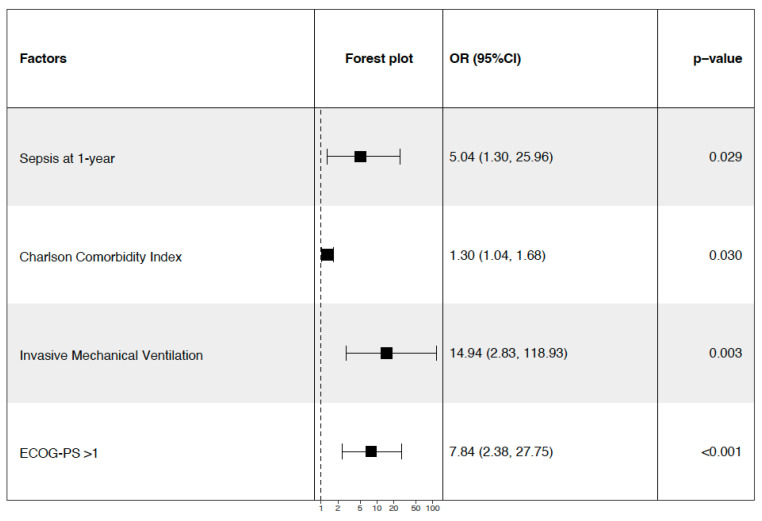
Background: Splenectomy remains necessary in selected oncologic and hematologic indications but is associated with significant postoperative morbidity and mortality. The data on outcomes in this high-risk population remain limited, particularly in mixed cohorts. Methods: We conducted a retrospective cohort study including all patients undergoing splenectomy for oncologic or hematologic causes between 2009 and 2022 at a cancer referral center. The primary outcomes were the occurrence of major complications at day 90 and the 1-year all-cause mortality. Multivariate logistic regression was used to identify independent predictors. Results: Among the 8503 ICU admissions from surgical wards, 204 splenectomies were performed; 179 patients were analyzed. The median age was 64 years, and 100 patients (55.9%) were female. Splenectomy was performed for hematologic malignancies in 76 cases (42.5%) and for oncologic causes in 103 cases (57.5%). Laparotomy was used in 154 cases (86.0%), and metastasectomy was performed in 54 patients (30.2%). At day 90, 86 patients (48.0%) developed a major complication: 12 deaths (6.7%), 44 surgical complications (24.6%), and 71 episodes of sepsis (39.7%). In a multivariate analysis, weight loss (OR 3.39, 95% CI [1.32-8.70], p = 0.011), laparotomy (OR 4.38 [1.09-17.60], p = 0.038), and a higher SAPS II score (OR 1.08 per point [1.03-1.13], p = 0.003) were associated with complications, while metastasectomy was protective (OR 0.23 [0.08-0.67], p = 0.007). At one year, the mortality reached 22.4%. Independent predictors of death were sepsis at one year (OR 5.04, 95% CI [1.30-25.96], p = 0.029), the Charlson Comorbidity Index (OR 1.30 per point, 95% CI [1.04-1.68], p = 0.030), invasive mechanical ventilation (OR 14.94, 95% CI [2.83-118.93], p = 0.003), and a performance status >1 (OR 7.84, 95% CI [2.38-27.75], p < 0.001). Encapsulated bacteria were not isolated; sepsis was mainly due to Gram-negative and enterococcal organisms. Conclusions: Splenectomy in onco-hematologic patients is associated with high rates of sepsis and mortality. In addition to surgical factors, frailty, immune status, and infection independently contribute to the patients' outcomes. These results support risk-adapted perioperative strategies and long-term infectious surveillance in immunocompromised patients.
Keywords: cancer; mortality; postoperative complications; postoperative sepsis; splenectomy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Kuter D.J., Ghanima W., Cooper N., Liebman H.A., Zhang L., Hu Y., Miyakawa Y., Homenda W., Morales Galindo L.E.E., Basquiera A.L., et al. Safety and Efficacy of Rilzabrutinib vs Placebo in Adults with Immune Thrombocytopenia: The Phase 3 LUNA3 Study. Blood. 2025;145:2914–2926. doi: 10.1182/blood.2024027336. - DOI - PubMed
-
- Mokart D., Giaoui E., Barbier L., Lambert J., Sannini A., Chow-Chine L., Brun J.-P., Faucher M., Guiramand J., Ewald J., et al. Postoperative Sepsis in Cancer Patients Undergoing Major Elective Digestive Surgery Is Associated with Increased Long-Term Mortality. J. Crit. Care. 2016;31:48–53. doi: 10.1016/j.jcrc.2015.10.001. - DOI - PubMed
-
- Yamashita K., Kurokawa Y., Yamamoto K., Hirota M., Kawabata R., Mikami J., Masuzawa T., Takiguchi S., Mori M., Doki Y. Risk Factors for Poor Compliance with Adjuvant S-1 Chemotherapy for Gastric Cancer: A Multicenter Retrospective Study. Ann. Surg. Oncol. 2017;24:2639–2645. doi: 10.1245/s10434-017-5923-2. - DOI - PubMed
LinkOut - more resources
Full Text Sources
