

Impact of a Surgical Approach on Endometrial Cancer Survival According to ESMO/ESGO Risk Classification: A Retrospective Multicenter Study in the Northern Italian Region
- PMID: 40647558
- PMCID: PMC12248672
- DOI: 10.3390/cancers17132261
Impact of a Surgical Approach on Endometrial Cancer Survival According to ESMO/ESGO Risk Classification: A Retrospective Multicenter Study in the Northern Italian Region
Abstract
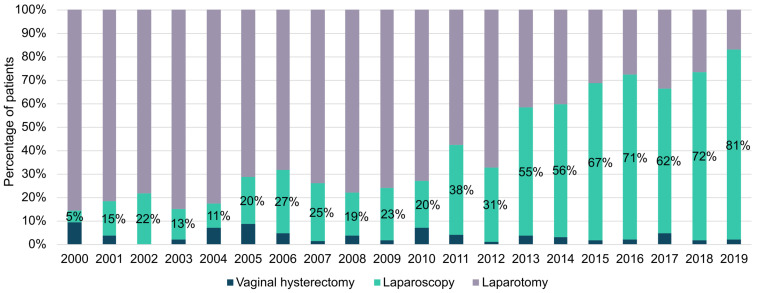
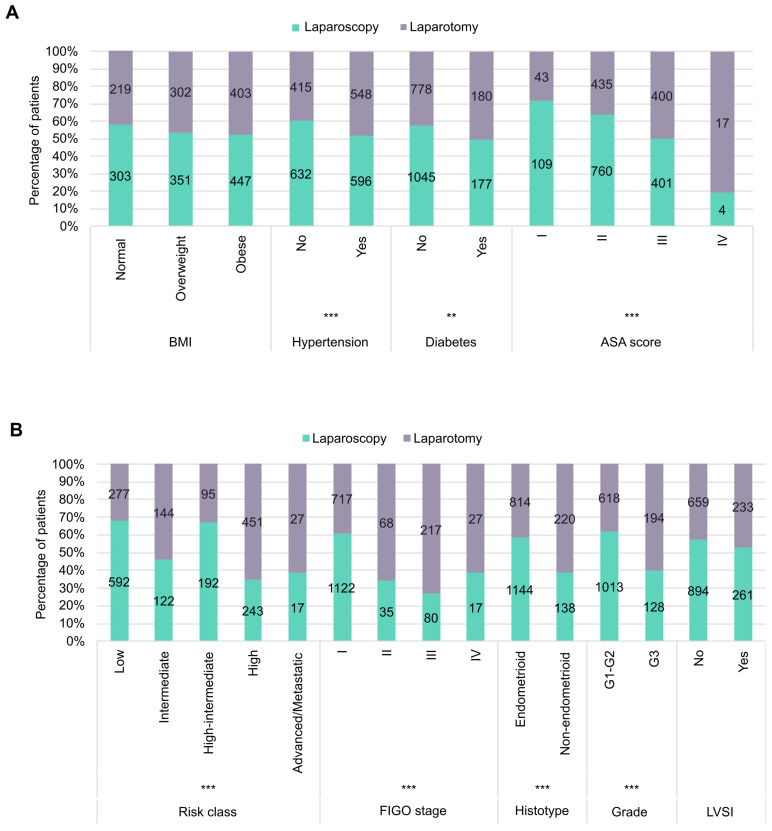
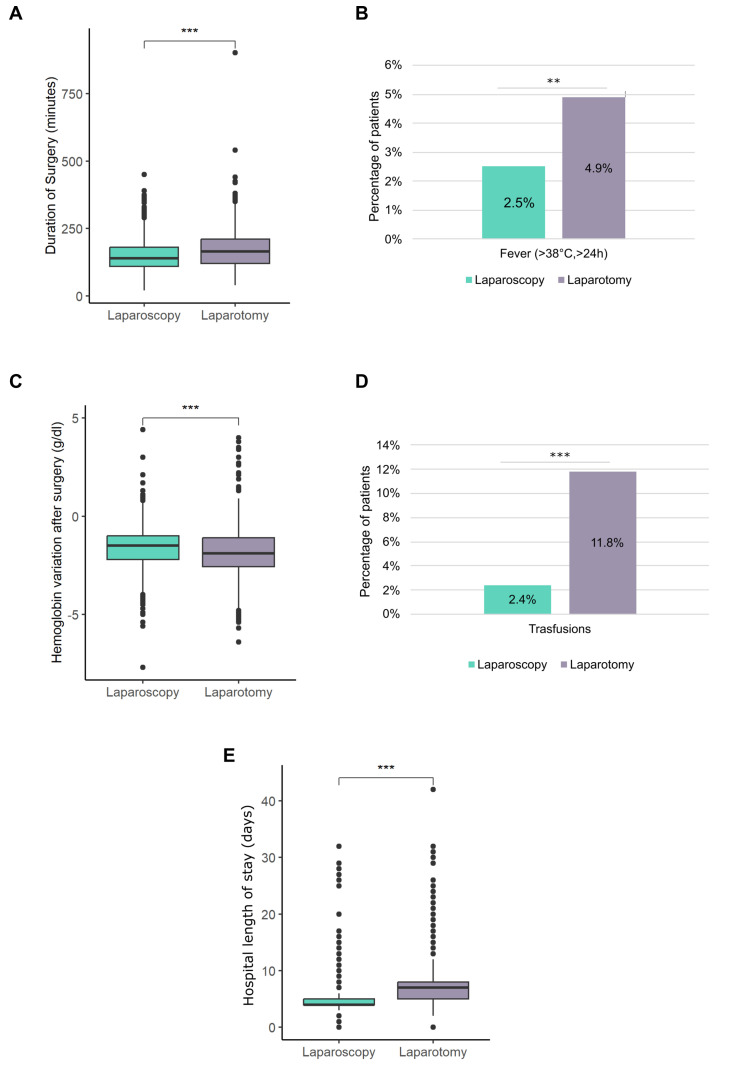
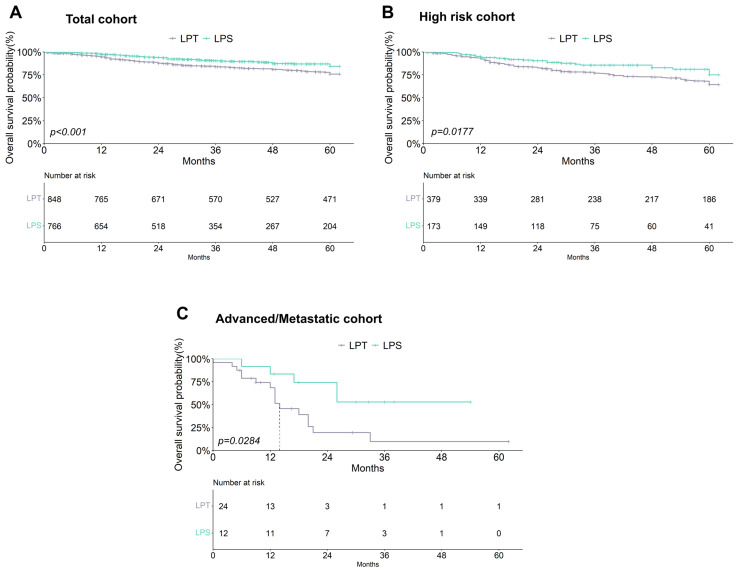
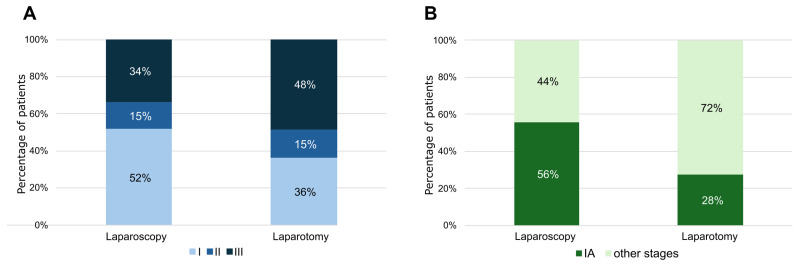
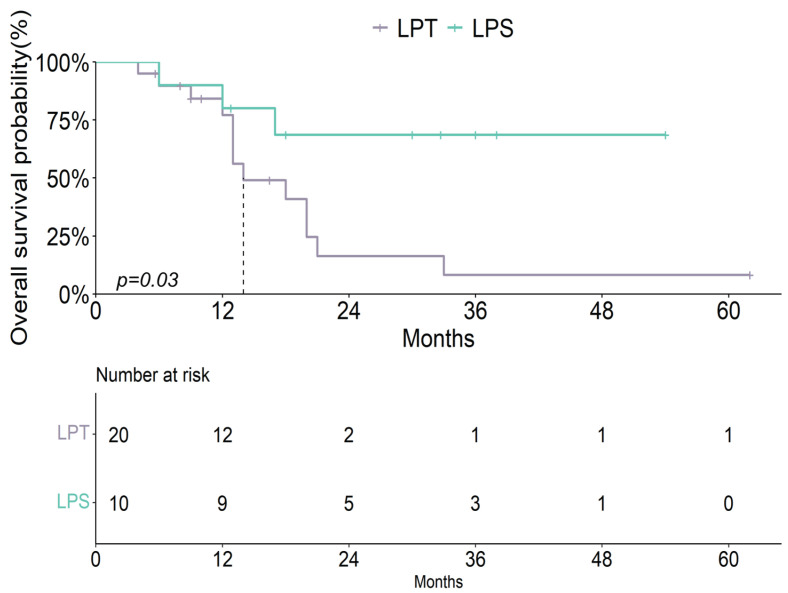
Background: Following the results of the Laparoscopic Approach to Carcinoma of the Cervix (LACC) trial, doubts have arisen about the safety of laparoscopy in the treatment of endometrial cancer. Methods: A retrospective multicenter cohort study which included all endometrial cancer (EC) patients who underwent a hysterectomy in Emilia Romagna hospitals from 2000 to 2019. All cases were revised and classified according to the 2009 International Federation of Gynaecology and Obstetrics (FIGO) staging system. The different impacts of the surgical approach on survival were stratified according to the recurrence risk from the 2016 European Society for Medical Oncology (ESMO)-European Society of Gynaecological Oncology (ESGO) classification system. The clinical characteristics and oncological outcome of patients treated by laparoscopy were compared with those treated by laparotomy. Results: A total of 2402 EC patients were included in the study. The use of laparoscopy has increased over the years, reaching 81% of procedures in 2019. Laparoscopy reduced complications and hospital stay. Laparoscopy was preferred to treat low, intermediate, and intermediate/high-risk patients. Laparoscopy showed no adverse effects on overall survival (OS) in any recurrence risk class. Particularly in high-risk EC patients, laparoscopy was associated with an increased OS in comparison with women treated by laparotomy regardless of the use of adjuvant therapy. Conclusions: Laparoscopy should always be chosen to treat EC of any risk class. The goal is to ensure correct treatment and oncological safety regardless of the surgical approach.
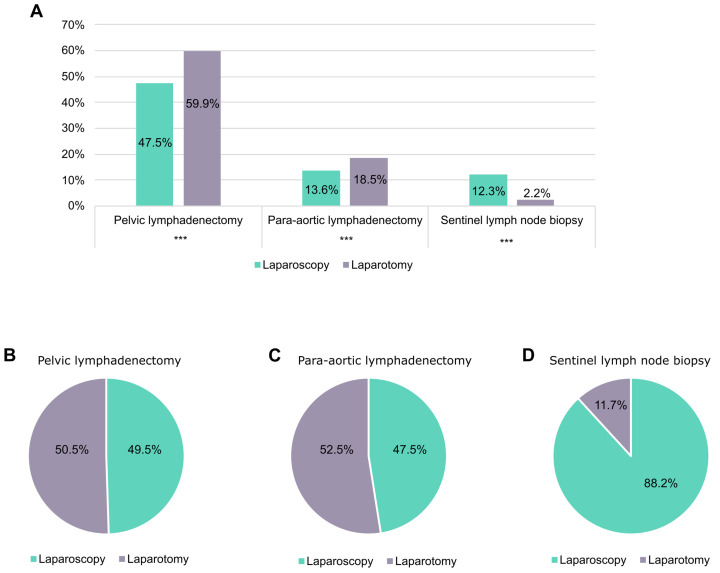
Keywords: ESMO-ESGO classification system; adjuvant therapy; endometrial cancers; high-risk endometrial cancer; laparoscopy; laparotomy; lymphadenectomy; sentinel lymph node biopsy; survival.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
Laparoscopy versus laparotomy for the management of early stage endometrial cancer.Cochrane Database Syst Rev. 2012 Sep 12;(9):CD006655. doi: 10.1002/14651858.CD006655.pub2. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2018 Oct 31;10:CD006655. doi: 10.1002/14651858.CD006655.pub3. PMID: 22972096 Updated.
-
Lymphadenectomy or sentinel node biopsy for the management of endometrial cancer.Cochrane Database Syst Rev. 2025 Jun 10;6(6):CD015786. doi: 10.1002/14651858.CD015786.pub2. Cochrane Database Syst Rev. 2025. PMID: 40492478 Review.
-
Lymphadenectomy for the management of endometrial cancer.Cochrane Database Syst Rev. 2017 Oct 2;10(10):CD007585. doi: 10.1002/14651858.CD007585.pub4. Cochrane Database Syst Rev. 2017. PMID: 28968482 Free PMC article.
-
Lymphadenectomy for the management of endometrial cancer.Cochrane Database Syst Rev. 2015 Sep 21;2015(9):CD007585. doi: 10.1002/14651858.CD007585.pub3. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2017 Oct 02;10:CD007585. doi: 10.1002/14651858.CD007585.pub4. PMID: 26387863 Free PMC article. Updated.
References
-
- American Cancer Society. [(accessed on 27 November 2024)]. Available online: https://www.cancer.org/cancer/types/endometrial-cancer/detection-diagnos....
-
- Chase D.M., Kobayashi M., Gomez P., Lubinga S.J., Chan J.K. Treatment patterns and out-comes by mismatch repair/microsatellite instability status among patients with primary advanced or recurrent endometrial cancer in the United States. Future Oncol. 2025;11:1–12. doi: 10.1080/14796694.2025.2516891. - DOI - PubMed
LinkOut - more resources
Full Text Sources
