

Comparing FIB-4, VCTE, pSWE, 2D-SWE, and MRE Thresholds and Diagnostic Accuracies for Detecting Hepatic Fibrosis in Patients with MASLD: A Systematic Review and Meta-Analysis
- PMID: 40647597
- PMCID: PMC12248751
- DOI: 10.3390/diagnostics15131598
Comparing FIB-4, VCTE, pSWE, 2D-SWE, and MRE Thresholds and Diagnostic Accuracies for Detecting Hepatic Fibrosis in Patients with MASLD: A Systematic Review and Meta-Analysis
Abstract
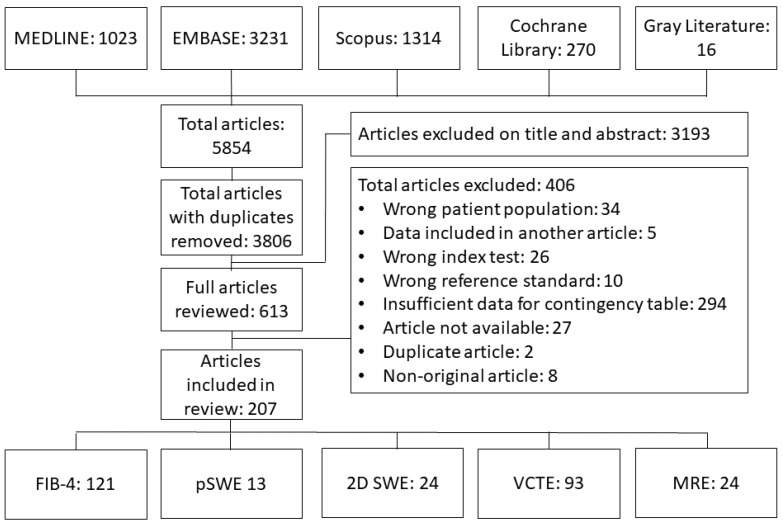
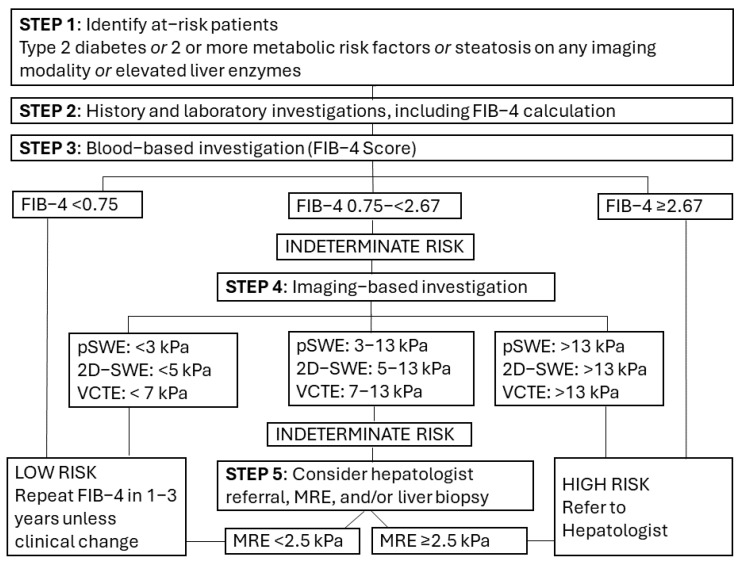
Objectives: To compare thresholds and accuracies of FIB-4, vibration-controlled transient elastography (VCTE), point shear wave elastography (pSWE), 2D shear wave elastography (2D-SWE), and MR elastography (MRE) for detecting hepatic fibrosis in patients with MASLD. Materials and Methods: Systematic searching of MEDLINE, EMBASE, Cochrane Library, Scopus, and the gray literature from inception to March 2024 was performed. Studies evaluating accuracies of FIB-4, VCTE, 2D-SWE, pSWE, and/or MRE for detecting significant (≥F2) and/or advanced (≥F3) hepatic fibrosis in MASLD patients compared to histology were identified. Full-text review and data extraction were performed independently by two reviewers. Multivariate meta-analysis and subgroup analyses were performed using index test and fibrosis grading. Risk of bias was assessed using QUADAS-2. Results: 207 studies with over 80,000 patient investigations were included. FIB-4 1.3 threshold sensitivity was 71% (95% CI 66-75%) for detecting advanced hepatic fibrosis, which improved to 88% (85-91%) using a <0.75 threshold. FIB-4 specificity using a 2.67 threshold was 96% (94-97%). Sensitivities of 88-91% were achieved using thresholds of 3.2 kPa for pSWE, 4.92 kPa for 2D-SWE, 7.18 kPa for VCTE, and 2.32 kPa for MRE. No significant differences were identified for sensitivities in subgroup analysis with thresholds between 7 and 9 kPa. Most imaging-based studies were high risk of bias for the index test. Conclusions: A FIB-4 threshold of <0.75 and modality-dependent thresholds (VCTE < 7 kPa; pSWE <3 kPa; 2D-SWE <5 kPa; and MRE <2.5 kPa) would achieve sensitivities of around 90% when defining low-risk MASLD in population screening. A modified two-tier algorithm aligning with existing Society of Radiologists in Ultrasound guidelines would improve risk stratification accuracies compared to existing guidelines by European and American liver societies.
Keywords: MASLD; MRE; SWE; accuracy; fibroScan; magnetic resonance elastography; metabolic dysfunction-associated steatotic liver disease; shear wave elastography; systematic review; transient elastography.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Tacke F., Horn P., Wong V.W.-S., Ratziu V., Bugianesi E., Francque S., Zelber-Sagi S., Valenti L., Roden M., Schick F., et al. EASL–EASD–EASO Clinical Practice Guidelines on the management of metabolic dysfunction-associated steatotic liver disease (MASLD) J. Hepatol. 2024;81:492–542. doi: 10.1016/j.jhep.2024.04.031. - DOI - PubMed
-
- Sterling R.K., Duarte-Rojo A., Patel K., Asrani S.K., Alsawas M., Dranoff J.A., Fiel M.I., Murad M.H., Leung D.H., Levine D., et al. AASLD Practice Guideline on imaging-based noninvasive liver disease assessment of hepatic fibrosis and steatosis. Hepatology. 2025;81:672–724. doi: 10.1097/HEP.0000000000000843. - DOI - PubMed
-
- Kanwal F., Shubrook J.H., Adams L.A., Pfotenhauer K., Wong V.W.-S., Wright E., Abdelmalek M.F., Harrison S.A., Loomba R., Mantzoros C.S., et al. Clinical Care Pathway for the Risk Stratification and Management of Patients with Nonalcoholic Fatty Liver Disease. Gastroenterology. 2021;161:1657–1669. doi: 10.1053/j.gastro.2021.07.049. - DOI - PMC - PubMed
-
- McInnes M.D.F., Moher D., Thombs B.D., McGrath T.A., Bossuyt P.M., Clifford T., Cohen J.F., Deeks J.J., Gatsonis C., Hooft L., et al. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies. The PRISMA-DTA Statement. JAMA. 2018;319:388–396. doi: 10.1001/jama.2017.19163. Erratum in JAMA 2019, 322, 2026. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
