

Quetiapine Use Is Associated with Longer ICU Stay Compared to Control and Haloperidol: A Propensity Score-Matched Analysis Using the MIMIC-IV Database
- PMID: 40648812
- PMCID: PMC12249598
- DOI: 10.3390/jcm14134438
Quetiapine Use Is Associated with Longer ICU Stay Compared to Control and Haloperidol: A Propensity Score-Matched Analysis Using the MIMIC-IV Database
Abstract
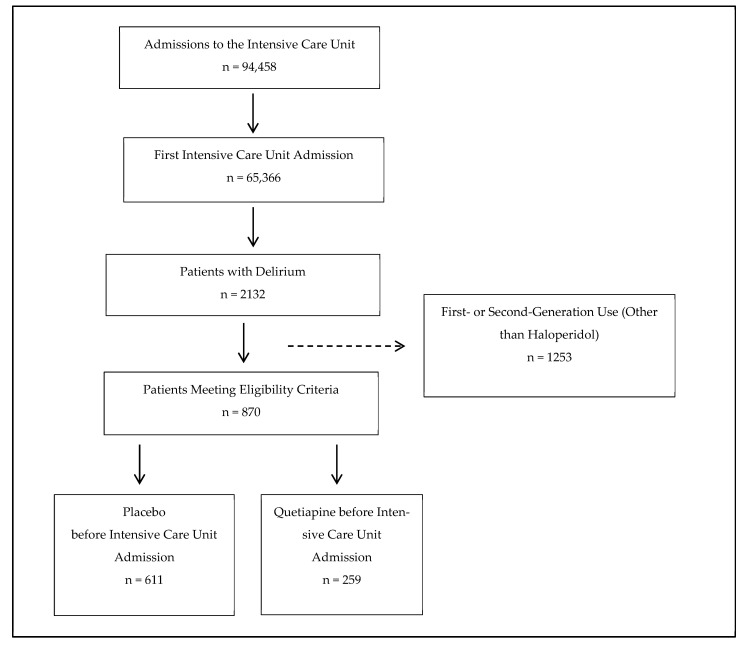
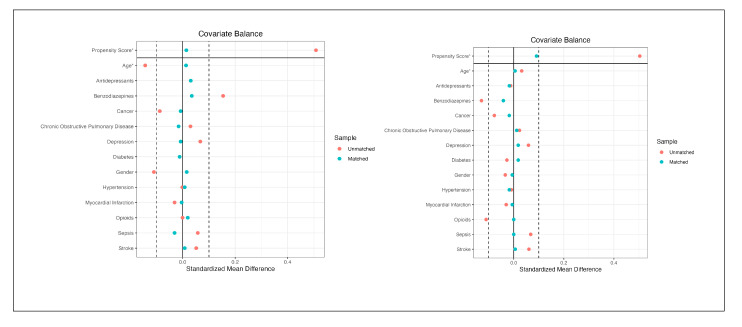
Background: Due to the low certainty of existing evidence, no formal recommendation can be made for or against the use of antipsychotics over usual care in ICU patients with delirium. To advance evidence-based practice, we used observational data from the Medical Information Mart for Intensive Care (MIMIC) to estimate the effect of pre-ICU quetiapine treatment (vs. control) on the length of ICU stay. In a second, head-to-head comparison, we assessed quetiapine vs. haloperidol on the same outcome. Methods: We conducted two propensity score-matched procedures: 518 patients were matched based on receipt of quetiapine versus no antipsychotic (i.e., control), and 336 patients based on quetiapine versus haloperidol prior to ICU admission. After matching, we performed Bayesian generalized additive modeling (GAM) and Bayesian sensitivity analyses within a nonlinear modeling framework. Results: In the quetiapine versus no quetiapine analysis, the original overall covariate distance of 0.48 was reduced to 0.01 post-matching. All covariates achieved an acceptable balance, with absolute standardized mean differences below 0.1. Quetiapine use was associated with a 1.31-day longer ICU stay (posterior mean = 0.36; 95% credible interval: 0.14 to 0.59). Sensitivity analyses indicated that this effect remained robust after accounting for plausible levels of unmeasured confounding. In the quetiapine versus haloperidol analysis, the initial overall distance of 0.40 was reduced to 0.09 after matching, with all covariates similarly balanced. Compared to haloperidol, quetiapine treatment was associated with a 1.46-day longer ICU stay (posterior mean = 0.48; 95% credible interval: 0.09 to 0.88). Bayesian sensitivity analyses again indicated the robustness of the effect estimate. Conclusions: In these emulated clinical trials, pre-ICU treatment with quetiapine was associated with a prolonged ICU stay compared to both untreated and haloperidol conditions. Though more research in this field is needed, these findings do not support the use of quetiapine in ICU patients with delirium.
Keywords: Medical Information Mart for Intensive Care; delirium; emulated clinical trial; haloperidol; intensive care unit; propensity score; quetiapine.
Conflict of interest statement
The author declares no conflicts of interest.
Figures
References
-
- Slooter A.J.C., Otte W.M., Devlin J.W., Arora R.C., Bleck T.P., Claassen J., Duprey M.S., Ely E.W., Kaplan P.W., Latronico N., et al. Updated Nomenclature of Delirium and Acute Encephalopathy: Statement of Ten Societies. Intensive Care Med. 2020;46:1020–1022. doi: 10.1007/s00134-019-05907-4. - DOI - PMC - PubMed
-
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; Washington, DC, USA: 2013.
LinkOut - more resources
Full Text Sources
