

Pain Relief, Disability, and Hospital Costs After Intradiscal Ozone Treatment or Microdiscectomy for Lumbar Disc Herniation: A 24-Month Real-World Prospective Study
- PMID: 40648907
- PMCID: PMC12250310
- DOI: 10.3390/jcm14134534
Pain Relief, Disability, and Hospital Costs After Intradiscal Ozone Treatment or Microdiscectomy for Lumbar Disc Herniation: A 24-Month Real-World Prospective Study
Abstract
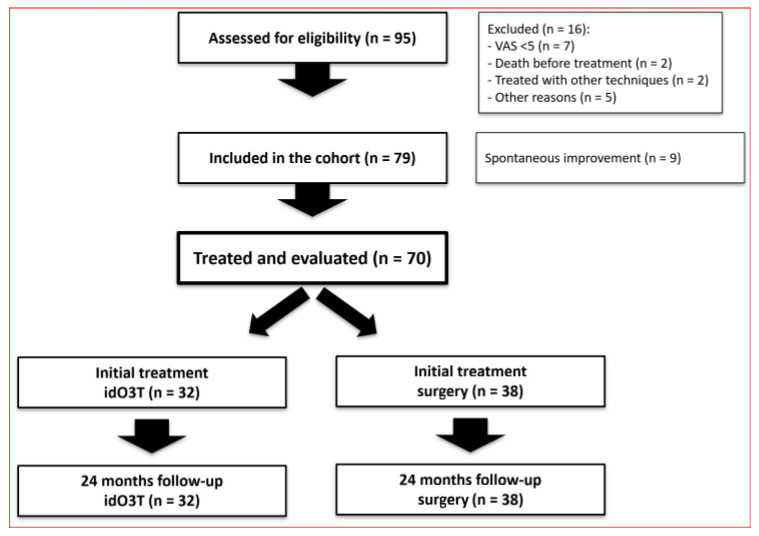
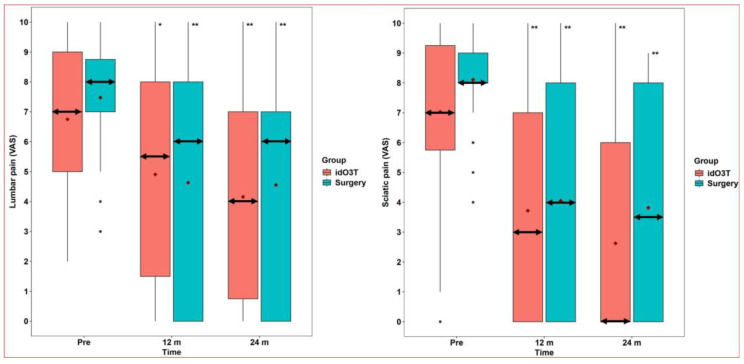
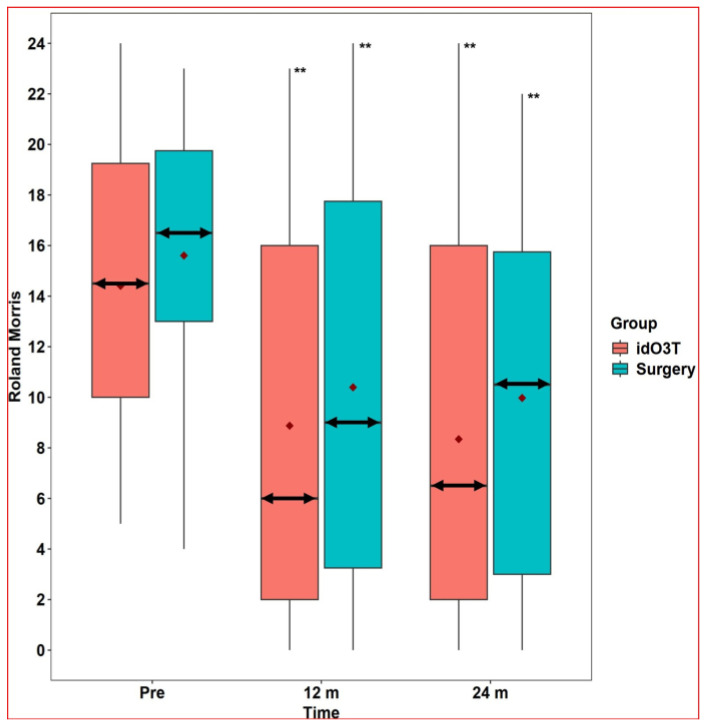
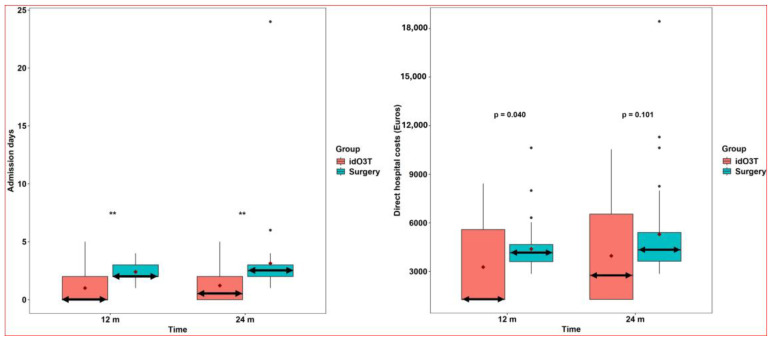
Background/Objectives: Surgery is the treatment of choice for symptomatic disc herniation after unsuccessful conservative management. This prospective study compared the impact on clinical and hospital outcomes of intradiscal ozone treatment vs. surgery (microdiscectomy/discectomy) in our clinical practice. Methods: Intradiscal ozone treatment was offered to 70 patients with scheduled surgery because of lumbar disc herniation. Initial treatment was surgery in 38 patients and ozone infiltration in 32 patients: lumbar and sciatic pain (Visual Analog Scale), Roland-Morris Disability Questionnaire score, days of hospital admission, and direct hospital costs were recorded during 24 months of follow-up. Results: At 12 and 24 months, lumbar pain, sciatic pain, and Roland-Morris score decreased significantly within both groups (p < 0.001). At 24 months, compared to the initial surgery, the initial intradiscal ozone treatment showed similar clinical outcomes with significantly lower requirements of surgery (100% versus 47%, p < 0.001) and lower hospital stay [median 2.5 (2-3) versus 0.5 (0-2) days, p < 0.001]. Direct hospital costs were significantly lower with initial ozone treatment at 12 months (p = 0.040). Conclusions: In our real-world prospective study, after 24 months of follow-up, initial intradiscal ozone treatment avoided surgery in more than half of patients and provided similar clinical outcomes with lower hospitalization requirements. In patients with lumbar disc herniation requiring surgery (microdiscectomy/discectomy), initial intradiscal ozone treatment could offer benefits for patients and healthcare service providers (NCT00566007).
Keywords: costs; disc herniation; discectomy or microdiscectomy; intradiscal ozone therapy; lumbar pain; radicular pain.
Conflict of interest statement
One ozone therapy device used in this study (Ozonosan Alpha-plus®) was provided by Renate Viebahn (Hänsler GmbH, Iffezheim, Germany). The other ozone therapy device used in this study (Ozonobaric-P, SEDECAL, Madrid, Spain) was supported by a grant (COV20/00702) from the Instituto de Salud Carlos III (Spanish Ministry of Science and Innovation, Madrid, Spain). In 2023, B.C. received financial support during a European grant application from Hänsler Medical GmbH (Iffezheim, Germany). The authors have no other financial interests to disclose.
Figures
Similar articles
-
Intradiscal oxygen-ozone chemonucleolysis versus microdiscectomy for lumbar disc herniation radiculopathy: a non-inferiority randomized control trial.Spine J. 2022 Jun;22(6):895-909. doi: 10.1016/j.spinee.2021.11.017. Epub 2021 Dec 9. Spine J. 2022. PMID: 34896609 Clinical Trial.
-
Comparison of discectomy with and without fusion in the surgical treatment of recurrent lumbar disc herniation.Neurosurg Rev. 2025 Jul 5;48(1):542. doi: 10.1007/s10143-025-03687-8. Neurosurg Rev. 2025. PMID: 40615773 Free PMC article.
-
Comparison of microdiscectomy and fragmentectomy on clinical outcomes for single level lumbar disc herniation: a systematic review and meta-analysis of comparative studies.J Clin Neurosci. 2025 Jun 25;139:111416. doi: 10.1016/j.jocn.2025.111416. Online ahead of print. J Clin Neurosci. 2025. PMID: 40570611 Review.
-
Effectiveness of intradiscal ozone injections for treating pain following herniated lumbar disc: A systematic review and meta-analysis.J Back Musculoskelet Rehabil. 2024;37(5):1131-1139. doi: 10.3233/BMR-240024. J Back Musculoskelet Rehabil. 2024. PMID: 38905033
-
Application of extracorporeal collagenase chemonucleolysis and combined intradiscal and extracorporeal collagenase chemonucleolysis via FLEX electrode in patients with lumbar disc herniation: a retrospective study.Eur Spine J. 2025 Jun 23. doi: 10.1007/s00586-025-09067-6. Online ahead of print. Eur Spine J. 2025. PMID: 40545511
References
-
- Safiri S., Kolahi A.A., Cross M., Hill C., Smith E., Carson-Chahhoud K., Mansournia M.A., Almasi-Hashiani A., Ashrafi-Asgarabad A., Kaufman J., et al. Prevalence, Deaths, and Disability-Adjusted Life Years Due to Musculoskeletal Disorders for 195 Countries and Territories 1990–2017. Arthritis Rheumatol. 2021;73:702–714. doi: 10.1002/art.41571. - DOI - PubMed
-
- Wu A., March L., Zheng X., Huang J., Wang X., Zhao J., Blyth F.M., Smith E., Buchbinder R., Hoy D. Global low back pain prevalence and years lived with disability from 1990 to 2017: Estimates from the Global Burden of Disease Study 2017. Ann. Transl. Med. 2020;8:299. doi: 10.21037/atm.2020.02.175. - DOI - PMC - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
