

Improving the Compliance of Massive Hemorrhage Protocols Through Education Is Associated with Patient Survival
- PMID: 40649007
- PMCID: PMC12250384
- DOI: 10.3390/jcm14134632
Improving the Compliance of Massive Hemorrhage Protocols Through Education Is Associated with Patient Survival
Abstract
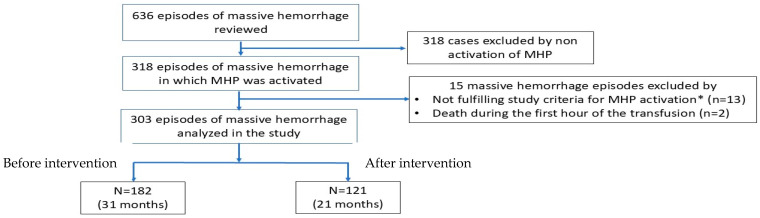
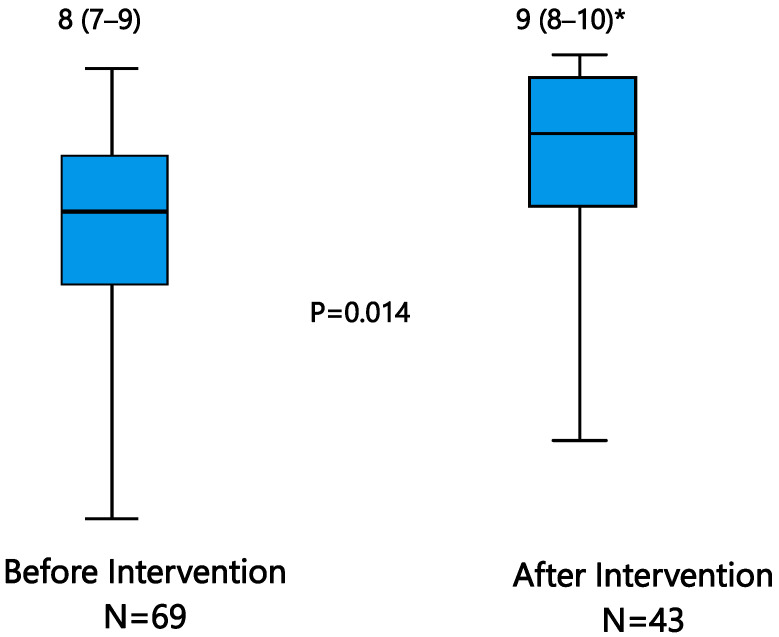
Background: In 2015, Spanish scientific societies published a consensus document on managing massive hemorrhage (MH). This study aimed to evaluate the knowledge and application of the Massive Hemorrhage Protocol (MHP) among healthcare professionals and to assess whether an educational intervention could improve compliance and patient outcomes. Methods: A two-phase observational study was conducted in four Spanish university hospitals. In phase one, compliance with MHP recommendations was surveyed. Based on the findings, educational sessions were implemented, focusing on the least known or followed recommendations. Compliance was then reassessed. Primary outcome was adherence to MHP; secondary outcomes included morbidity and 24 h and in-hospital mortality. Results: The MHP was activated in 303 MH episodes, mostly of surgical (42.6%) or traumatic (25%) origin. The most followed recommendation before the intervention was protocol activation (94%), which improved to 98.3% post-intervention (p = 0.049). Lesser-followed recommendations such as requesting a hemorrhage lab panel and correcting hypothermia improved after intervention from 39% to 50.4% (p = 0.05) and 31.3% to 43.8% (p = 0.027), respectively. Overall compliance increased from 68% to 73% (p = 0.05). Mortality remained high in both phases, 24 h (25.4%) and in-hospital (42.2%). Patients who required massive transfusion had higher mortality (53.6%) than those who did not (35.9%, p = 0.03). Survivors had higher protocol compliance (p = 0.003 at 24 h; p = 0.049 in-hospital). Conclusions: Educational intervention modestly improved adherence to MHP recommendations. Higher compliance was associated with better survival outcomes, supporting the need for targeted educational strategies to enhance protocol implementation and improve care in MH cases.
Keywords: education; massive hemorrhage; mortality; protocol compliance.
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
References
-
- Etchill E., Sperry J., Zuckerbraun B., Alarcon L., Brown J., Schuster K., Kaplan L., Piper G., Peitzman A., Neal M.D. The confusion continues: Results from an American Association for the Surgery of Trauma survey on massive transfusion practices among United States trauma centers. Transfusion. 2016;56:2478–2486. doi: 10.1111/trf.13755. - DOI - PubMed
-
- Holcomb J., Caruso J., McMullin N., Wade C.E., Pearse L., Oetjen-Gerdes L., Champion H.R., Lawnick M., Farr W., Rodriguez S., et al. Causes of death in U.S. special operations forces in the global war on terrorism: 2001–2004. Ann. Surg. 2007;245:986–991. doi: 10.1097/01.sla.0000259433.03754.98. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
