

Evaluating an Early Risk Model for Uncomplicated Hypertension in Pregnancy Based on Nighttime Blood Pressure, Uric Acid, and Angiogenesis-Related Factors
- PMID: 40649890
- PMCID: PMC12249693
- DOI: 10.3390/ijms26136115
Evaluating an Early Risk Model for Uncomplicated Hypertension in Pregnancy Based on Nighttime Blood Pressure, Uric Acid, and Angiogenesis-Related Factors
Abstract
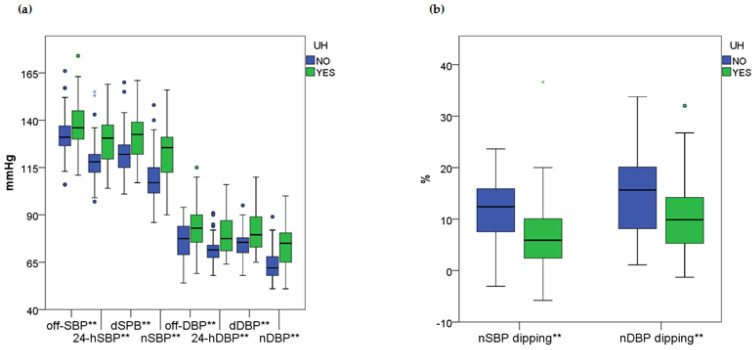
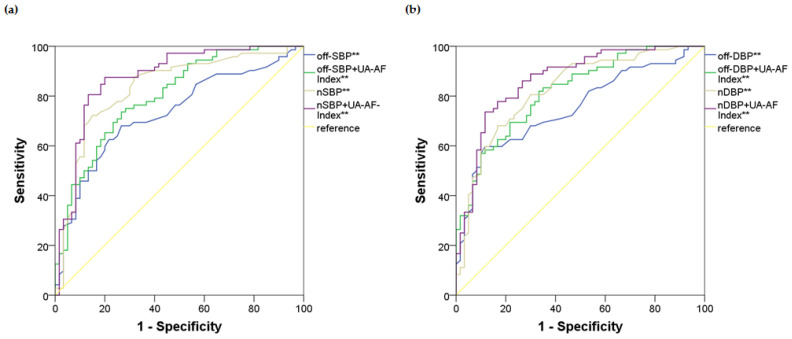
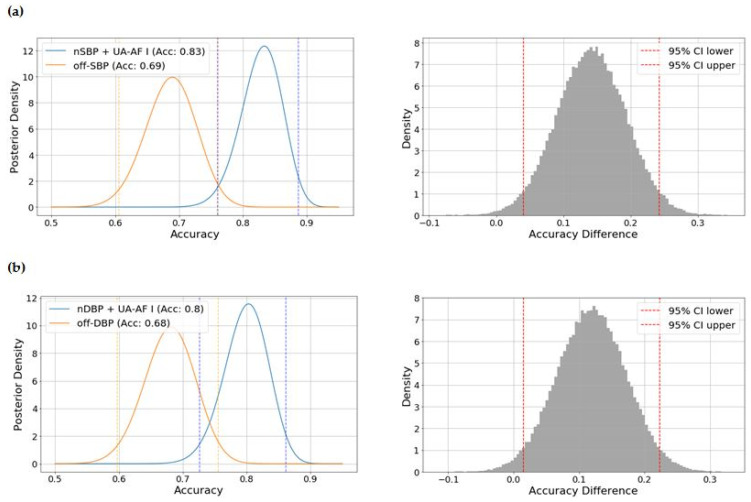
Uncomplicated hypertension (UH) during pregnancy represents a common condition, worsening maternal and fetal prognosis. However, no single biomarker has proven optimal for determining the risk of UH. We developed an early risk multivariate model for UH, integrating hemodynamics with biochemistry, focusing on the relationship between blood pressure (BP) indices, uric acid (UA), and angiogenesis-related factors (AF). We collected and analyzed data on 24 h ambulatory BP monitoring, demographic, epidemiological, clinical, and laboratory variables from 132 pregnancies. The main predictors were BP indices and serum UA and AF levels. Uncomplicated hypertension, defined as the presence of gestational hypertension or worsening of essential hypertension beyond the 20th week, was the main outcome. The combined second-degree polynomial transformation of UA and the AF (sFlt-1/PIGF) ratio, called the UA-AF Index, consistently showed a positive association with UH. The models incorporating nighttime BP indices combined with the UA-AF Index outperformed the others, with the best-performing model based on the nocturnal systolic BP (SBP). Specifically, in the best-fitting model (nighttime SBP + UA-AF Index as predictors), each 1 mmHg increase in nocturnal SBP was associated with a 10% higher risk of UH, while each one-unit increase in the UA-AF Index raised the likelihood of UH by more than twofold (accuracy: 0.830, AUC 0. 874, SE 0.032, p-value < 0.001, 95%CI 0.811-0.938). The combination of nighttime blood pressure indices, serum uric acid, and angiogenesis-related factors may provide added value in the assessment of uncomplicated hypertension during pregnancy.
Keywords: angiogenesis; blood pressure; gestational; hypertension; monitoring; nighttime; pregnancy; uric acid.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Penny J.A., Halligan A.W., Shennan A.H., Lambert P.C., Jones D.R., de Swiet M., Taylor D.J. Automated, ambulatory, or conventional blood pressure measurement in pregnancy: Which is the better predictor of severe hypertension? Am. J. Obstet. Gynecol. 1998;178:521–526. doi: 10.1016/S0002-9378(98)70432-6. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
