

Radiation-induced temporal lobe necrosis in a nasopharyngeal cancer patient after external beam radiotherapy: a case report and review of literature
- PMID: 40652209
- PMCID: PMC12255967
- DOI: 10.1186/s13256-025-05368-y
Radiation-induced temporal lobe necrosis in a nasopharyngeal cancer patient after external beam radiotherapy: a case report and review of literature
Abstract
Background: Nasopharyngeal carcinoma is considered rare worldwide. The treatment of nasopharyngeal carcinoma primarily relies on radiotherapy, as the tumor cells in NPC exhibit radiosensitivity. However, excessive dosage can result in a delayed reaction that affects the healthy surrounding tissues, including the central nervous system, causing brain radionecrosis, a rare yet severe condition, which can develop approximately 6-12 months after radiation as a significant complication. The majority of studies on brain radionecrosis have been conducted in China, where nasopharyngeal carcinoma is most prevalent. However, to the best of our knowledge, this is the first reported case of brain radionecrosis following radiotherapy for nasopharyngeal carcinoma in our region, which was diagnosed using magnetic resonance spectroscopy.
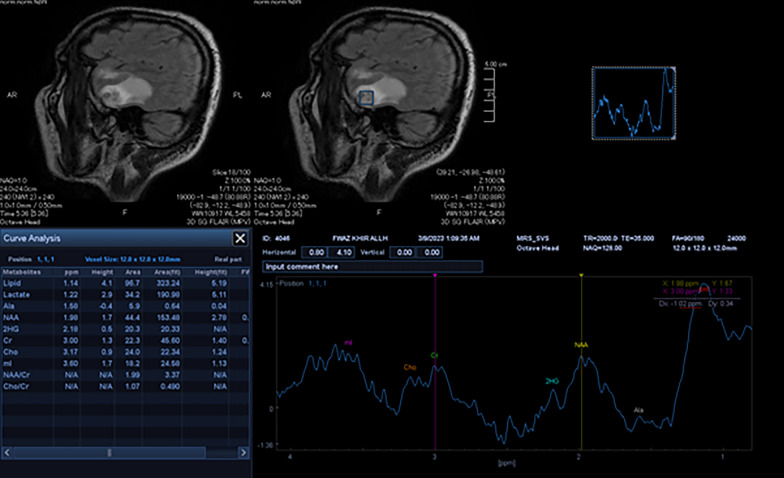
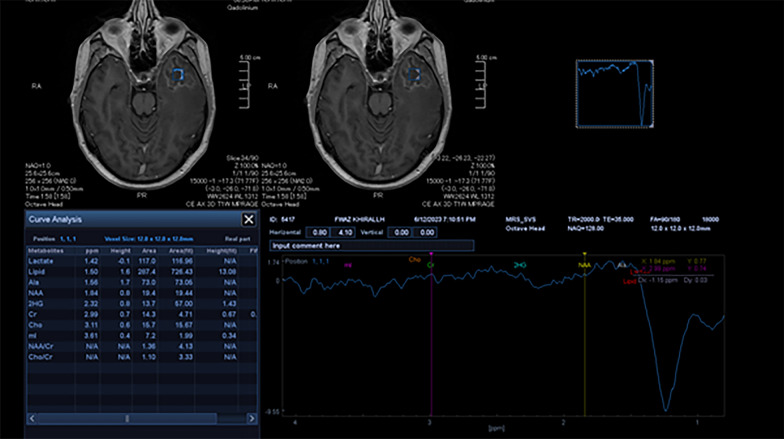
Case presentation: This case report describes a 49-year-old Arab male who presented with memory loss, expressive aphasia, and delirium 5 months after undergoing radiotherapy with a total radiation dose of 66 Gray for nasopharyngeal carcinoma (NPC). Magnetic resonance imaging with magnetic resonance spectroscopy revealed the presence of focal lesions in the left temporal lobe with accompanying brain edema indicative of radionecrosis.
Conclusion: It is imperative to consider the possibility of brain radionecrosis in patients who have previously received radiation therapy for head and neck cancers, particularly nasopharyngeal carcinoma. Early detection of brain radionecrosis is essential, and diagnostic imaging should be performed regularly during follow-up using magnetic resonance imaging and magnetic resonance spectroscopy. The primary objective of treatment is to alleviate symptoms through medical and/or surgical interventions.
Keywords: Cerebral radiation necrosis; Nasopharyngeal carcinoma; Radionecrosis; Radiotherapy; Temporal lobe necrosis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal. Competing interests: The authors declare that they have no competing interests.
Figures


References
-
- Ruben JD, Dally M, Bailey M, Smith R, McLean CA, Fedele P. Cerebral radiation necrosis: incidence, outcomes, and risk factors with emphasis on radiation parameters and chemotherapy. Int J Radiat Oncol. 2006;65(2):499–508. - PubMed
-
- Cross NE, Glantz MJ. Neurologic complications of radiation therapy. Neurol Clin. 2003;21(1):249–77. - PubMed
-
- Travers S, Joshi K, Miller DC, Singh A, Nada A, Biedermann G, et al. Reliability of magnetic resonance spectroscopy and positron emission tomography computed tomography in differentiating metastatic brain tumor recurrence from radiation necrosis. World Neurosurg. 2021;151:e1059-68. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
