

Matching-adjusted indirect comparison of enzalutamide versus darolutamide doublet in mHSPC
- PMID: 40654300
- PMCID: PMC12330274
- DOI: 10.1080/14796694.2025.2526324
Matching-adjusted indirect comparison of enzalutamide versus darolutamide doublet in mHSPC
Abstract
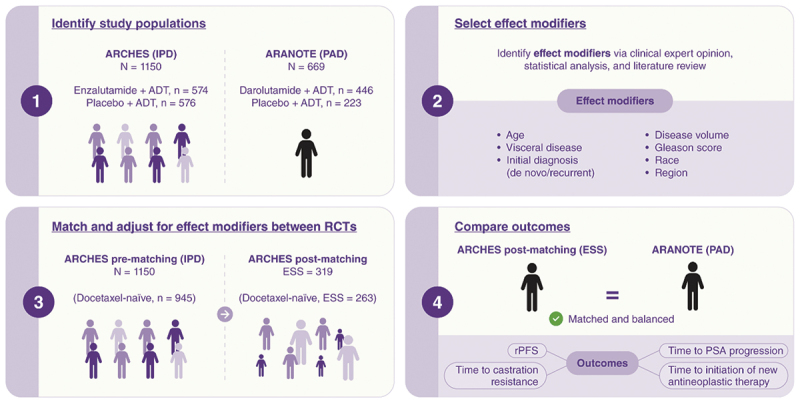
Aims: To compare the efficacy of enzalutamide + androgen-deprivation therapy (ADT) versus darolutamide + ADT for treatment of patients with metastatic hormone-sensitive prostate cancer (mHSPC) using a matching-adjusted indirect comparison (MAIC).
Patients and methods: Individual patient data from ARCHES (NCT02677896; enzalutamide + ADT, N = 1150) were weighted and adjusted to match published aggregated data on baseline characteristics from ARANOTE (NCT04736199; darolutamide + ADT, N = 669). The MAIC was anchored on the common comparator, placebo + ADT, and provided a (matching-adjusted) hazard ratio (HR) of enzalutamide versus darolutamide.
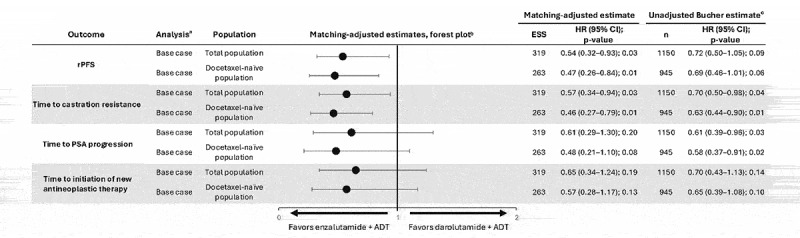
Results: Treatment with enzalutamide + ADT significantly prolonged the primary endpoint of radiographic progression-free survival (HR [95% confidence interval, CI]: 0.54 [0.32-0.93], p = 0.03) and time to castration resistance (HR [95% CI]: 0.57 [0.34-0.94], p = 0.03) compared with darolutamide + ADT (effective sample size: 319). Time to prostate-specific antigen progression (HR [95% CI]: 0.61 [0.29-1.30], p = 0.20) and time to initiation of new antineoplastic therapy (HR [95% CI]: 0.65 [0.34-1.24], p = 0.19) favored enzalutamide over darolutamide, albeit the difference was not statistically significant.
Conclusions: Enzalutamide + ADT showed better efficacy than darolutamide + ADT for treatment of patients with mHSPC. These findings can help inform treatment decisions in clinical practice.
Keywords: Androgen receptor pathway inhibitor; darolutamide; enzalutamide; indirect treatment comparison; metastatic hormone-sensitive prostate cancer.
Plain language summary
What is this article about?Metastatic prostate cancer is a form of prostate cancer that has spread beyond the prostate to other parts of the body. Androgen-deprivation therapy is a form of therapy that can stop or slow down the growth of metastatic prostate cancer by reducing testosterone levels. When prostate cancer responds to androgen-deprivation therapy, it is known as hormone-sensitive or castration-sensitive prostate cancer. When androgen-deprivation therapy stops working, it is known as castration-resistant prostate cancer.Enzalutamide and darolutamide are hormone treatments used for metastatic hormone-sensitive prostate cancer. We wanted to know if enzalutamide or darolutamide, when combined with androgen-deprivation therapy, was more efficacious in delaying how long it took patients with metastatic hormone-sensitive prostate cancer to get worse. Since there are no clinical trials that directly compare enzalutamide to darolutamide, we conducted a matching-adjusted indirect comparison of two different trials of patients with metastatic hormone-sensitive prostate cancer taking androgen-deprivation therapy combined with enzalutamide (ARCHES trial) or darolutamide (ARANOTE trial).What were the results of the study?It took longer for prostate cancer to get worse (progress further or lead to death) and to become castration-resistant in patients with metastatic hormone-sensitive prostate cancer who took enzalutamide with androgen-deprivation therapy compared to patients who took darolutamide with androgen-deprivation therapy. This difference in efficacy was considered clinically significant.What do the results of the study mean?These findings may have an impact on treatment decision-making in patients with metastatic hormone-sensitive prostate cancer.
Conflict of interest statement
AJA reports having received study funding and support for medical writing/editing from Astellas; consulting fees from Astellas, AstraZeneca, Bayer, Bristol Myers Squibb, Clovis, Dendreon, Merck, and Pfizer; payment or honoraria for lectures, presentations, speakers’ bureaus, publication writing or educational events from Astellas; support for attending meetings and/or travel from Astellas; research funding from Astellas, AstraZeneca, Bayer, BeiGene, Dendreon, Bayer, Bristol Myers Squibb, Constellation, Gilead, Janssen, Merck, Novartis, Pfizer, and Genentech; has participated on a Data Safety Monitoring Board or Advisory Board for Astellas, AstraZeneca, Bayer, Bristol Myers Squibb, Clovis, Dendreon, Merck, and Pfizer; and has a patent planned, issued, or pending for circulating tumor cell novel capture technology.
BJP is an employee of Astellas Pharma Inc. and is a board member of Sky Schools.
HSB is an employee of Astellas Pharma Inc.
AG is an employee of Astellas Pharma Inc. and holds stocks in AbbVie Inc.
VD is an employee of IQVIA.
AM is an employee of IQVIA.
AAA reports having received study funding and support for medical writing/editing from Astellas; consulting fees from Amgen, Astellas, AstraZeneca, Bayer, Bristol Myers Squibb, Ipsen, Janssen, Merck, Merck Serono, Novartis, Noxopharm, Sanofi, Telix, and Tolmar; payment or honoraria for lectures, presentations, publication writing or educational events from Amgen, Arvinas, Astellas, AstraZeneca, Bayer, Bristol Myers Squibb, Daiichi Sankyo, Ipsen, Janssen, Merck Serono, Merck Sharp & Dohme, Noxopharm, Novartis, Pfizer, Sanofi, Telix, and Tolmar; payment or honoraria for speakers’ bureaus from Amgen, Astellas, Bayer, Bristol Myers Squibb, Ipsen, Janssen, Merck Serono, and Novartis; support for attending meetings and/or travel from Amgen, Astellas, Bayer, Janssen, Hinova, Merck Serono, Pfizer, Sanofi, and Tolmar; research funding from Aptevo, Astellas, AstraZeneca, Bionomics, Bristol Myers Squibb, GlaxoSmithKline, Ipsen, MedImmune, Merck Serono, Novartis, Pfizer, Sanofi, and Synthorx; and has participated on a Data Safety Monitoring Board or Advisory Board for Amgen, Astellas, AstraZeneca, Bayer, Bristol Myers Squibb, Daiichi Sankyo, Ipsen, Janssen, Merck, Merck Serono, Novartis, Noxopharm, Sanofi, Telix, and Tolmar.
The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in, or financial conflict with, the subject matter or materials discussed in the manuscript, apart from those disclosed.
Figures
References
-
- Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Prostate Cancer V.2.2025. © National Comprehensive Cancer Network, Inc; 2025. All rights reserved [cited 2025 Apr 23]. All rights reserved.
-
- European Association of Urology . EAU - EANM - ESTRO - ESUR - ISUP - SIOG Guidelines on prostate cancer. 2024. [cited 2025 Apr 16]. Available from: https://d56bochluxqnz.cloudfront.net/documents/full-guideline/EAU-EANM-E...
-
- Armstrong AJ, Szmulewitz RZ, Petrylak DP, et al. ARCHES: a randomized, phase III study of androgen deprivation therapy with enzalutamide or placebo in men with metastatic hormone-sensitive prostate cancer. J Clin Oncol. 2019;37(32):2974–2986. doi: 10.1200/JCO.19.00799 - DOI - PMC - PubMed
-
•• This primary analysis of the phase 3, ARCHES randomized controlled trial demonstrated that enzalutamide plus androgen-deprivation therapy (ADT) significantly reduced the risk of radiographic progression or death compared to placebo plus ADT in patients with metastatic hormone-sensitive prostate cancer. ARCHES data served as the independent patient data included in the current matching-adjusted indirect comparison.
-
- Saad F, Vjaters E, Shore N, et al. Darolutamide in combination with androgen-deprivation therapy in patients with metastatic hormone-sensitive prostate cancer from the phase III ARANOTE trial. J Clin Oncol. 2024;42(36):4271–4281. doi: 10.1200/JCO-24-01798 - DOI - PMC - PubMed
-
•• The phase 3, ARANOTE randomized controlled trial demonstrated that darolutamide plus androgen-deprivation therapy (ADT) significantly reduced the risk of radiographic progression or death compared with placebo plus ADT in men with metastatic hormone-sensitive prostate cancer. ARANOTE data served as the published aggregate data included in the current matching-adjusted indirect comparison.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical