

Dynamic contrast-enhanced magnetic resonance imaging of masticatory muscles in patients with idiopathic condylar resorption
- PMID: 40654406
- PMCID: PMC12254837
- DOI: 10.1016/j.jds.2025.04.031
Dynamic contrast-enhanced magnetic resonance imaging of masticatory muscles in patients with idiopathic condylar resorption
Abstract
Background/purpose: Idiopathic condylar resorption (ICR), a subset of temporomandibular disorders (TMDs), presents an unclear relationship between structural changes in the mandibular condyle and alterations in masticatory muscle perfusion. This study aimed to investigate the correlation between mandibular condyle structural changes and masticatory muscle perfusion in patients with ICR using dynamic contrast-enhanced (DCE) magnetic resonance imaging (MRI).
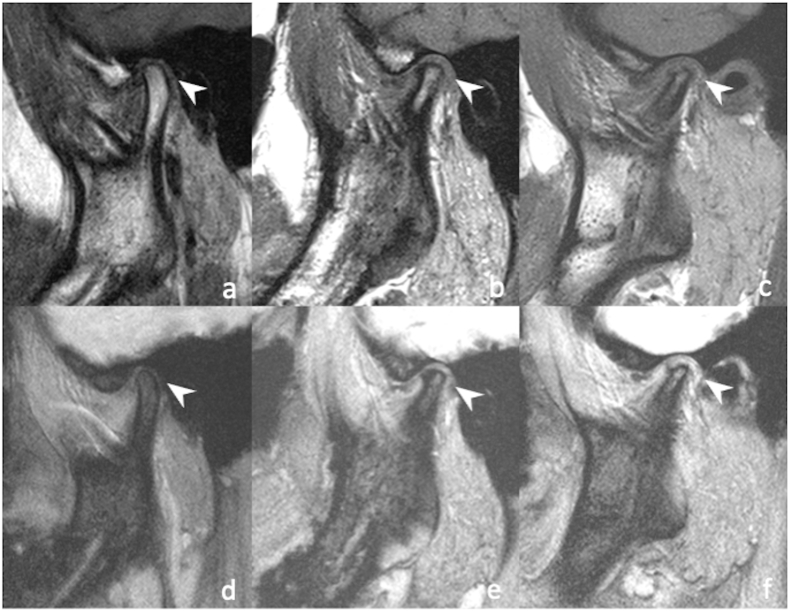
Materials and methods: From July 2018 to August 2022, patients with ICR from hospital-based TMD clinics underwent conventional and DCE MRI examinations. The patients were categorized on the basis of the degree of temporomandibular joint (TMJ) condylar resorption into grade 0 (normal), grade 1 (mild to moderate), and grade 2 (severe). DCE MRI parameters of masticatory muscles responsible for mouth closing (masseter [MA] and medial pterygoid [MP]) and opening (lateral pterygoid [LP]) were examined.
Results: Among 79 patients (158 TMJs), 41 % were assigned to the grade 0 group, 29 % were assigned to the grade 1 group, and 30 % were assigned to the grade 2 group. No significant differences in demographic or physical parameters were observed between the groups. In cases of severe condylar resorption (grade 2), the LP muscle exhibited a marked increase in plasma volume; none of the other muscles exhibited significant variations in plasma volume.
Conclusion: Increased plasma volume perfusion of the LP muscle is correlated with the severity of TMJ condylar resorption, indicating a specific correlation between muscle function and ICR severity. DCE MRI is useful for exploring muscular adaptation in patients with ICR and TMDs.
Keywords: Dynamic contrast enhanced magnetic resonance imaging; Idiopathic condylar resorption; Mandibular condyle; Masticatory muscles; Temporomandibular joint disorders.
© 2025 Association for Dental Sciences of the Republic of China. Publishing services by Elsevier B.Vé.
Conflict of interest statement
The authors have no conflicts of interest relevant to this article.
Figures



Similar articles
-
Magnetic Resonance Imaging of Submental and Masticatory Muscle Morphology and Its Relationship with Temporomandibular Joint Structures.Diagnostics (Basel). 2025 Jun 17;15(12):1535. doi: 10.3390/diagnostics15121535. Diagnostics (Basel). 2025. PMID: 40564855 Free PMC article.
-
The relationship between the articular disc in magnetic resonance imaging and the condyle in cone beam computed tomography: A retrospective study.J Stomatol Oral Maxillofac Surg. 2024 Sep;125(12 Suppl 2):101940. doi: 10.1016/j.jormas.2024.101940. Epub 2024 Jun 8. J Stomatol Oral Maxillofac Surg. 2024. PMID: 38857693
-
[Clinical analysis of changes in the position of the condyle and temporomandibular joint after repair of mandibular defects].Hua Xi Kou Qiang Yi Xue Za Zhi. 2025 Jun 1;43(3):422-430. doi: 10.7518/hxkq.2025.2024337. Hua Xi Kou Qiang Yi Xue Za Zhi. 2025. PMID: 40523823 Free PMC article. Chinese.
-
Magnetic resonance perfusion for differentiating low-grade from high-grade gliomas at first presentation.Cochrane Database Syst Rev. 2018 Jan 22;1(1):CD011551. doi: 10.1002/14651858.CD011551.pub2. Cochrane Database Syst Rev. 2018. PMID: 29357120 Free PMC article.
-
Association between clinical symptoms and MRI image findings in symptomatic temporomandibular joint (TMJ) disease: A systematic review.J Craniomaxillofac Surg. 2024 Jul;52(7):835-842. doi: 10.1016/j.jcms.2024.04.006. Epub 2024 Apr 27. J Craniomaxillofac Surg. 2024. PMID: 38724287
References
-
- Schiffman E., Ohrbach R., Truelove E., et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for clinical and research applications: recommendations of the international RDC/TMD consortium network∗ and orofacial pain special interest group†. J Oral Facial Pain Headache. 2014;28:6–27. - PMC - PubMed
-
- Mitsimponas K., Mehmet S., Kennedy R., Shakib K. Idiopathic condylar resorption. Br J Oral Maxillofac Surg. 2018;56:249–255. - PubMed
-
- Posnick J.C., Fantuzzo J.J. Idiopathic condylar resorption: current clinical perspectives. J Oral Maxillofac Surg. 2007;65:1617–1623. - PubMed
-
- Arnett G.W., Gunson M.J. Risk factors in the initiation of condylar resorption. Semin Orthod. 2013;19:81–88.
LinkOut - more resources
Full Text Sources
