

The Potential Effect of Dapagliflozin and Liraglutide in Attenuating Cardio-Renal Injuries in Diabetic Rats
- PMID: 40655462
- PMCID: PMC12248737
- DOI: 10.2147/JEP.S522053
The Potential Effect of Dapagliflozin and Liraglutide in Attenuating Cardio-Renal Injuries in Diabetic Rats
Abstract
Objective: To evaluate the therapeutic benefits of dapagliflozin and liraglutide as treatments for type 2 diabetes mellitus and their combined effects on T2DM-related complications, specifically cardio-renal injury.
Methods: Thirty rats were randomly allocated into two groups, with the first group serving as the control group, which had 6 rats. The second group was the experimental group, which had 24 rats administered a high-fat diet for four weeks, followed by a single dose of streptozotocin (STZ) to induce diabetes mellitus (DM). This, combined with a high-fat diet, a low dose of STZ was used to cause sub-lethal damage to beta cells. HFD/STZ is an easy method to successfully create a rat model resembling human T2DM, causing insulin resistance, but it does not fully capture the complexity of human T2DM. The experimental group was randomly divided into a positive control group, a liraglutide (0.4 mg/kg, s.c) group, a dapagliflozin (1 mg/kg, orally) group, and a combination of Dapa and lira group, which were administered daily for four weeks. Blood samples were analyzed for glucose, insulin, and cardiac and kidney function markers. Cardiac and kidney tissue were examined to assess redox balance, glutathione (GSH), catalase (CAT), and malondialdehyde (MDA).
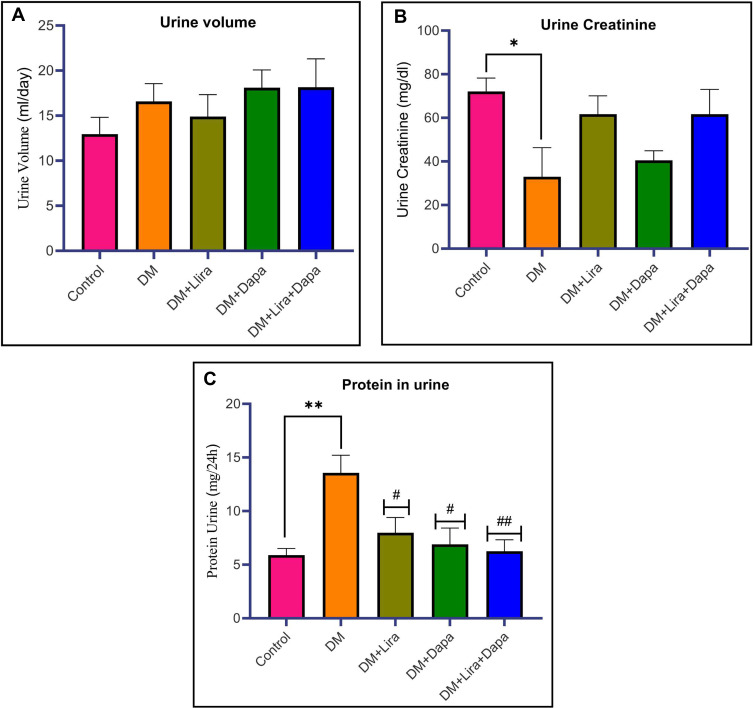
Results: Dapa and/or lira administration improved the body weight, lipid profile, cardiac and kidney function markers. Furthermore, all treating groups exhibited restoration of the balance between oxidants and antioxidants. Histological studies also revealed a reduction in cardiorenal tissue injury caused by diabetes. Interestingly, the combined management of Dapa and Lira showed a more beneficial protective effect than individual treatments. This study uniquely explores the simultaneous impact on cardiac and renal systems in a diabetic model, offering novel insights into cardiorenal interaction and the combined therapeutic potential of Dapa and Lira.
Conclusion: These findings suggest that the combination of dapagliflozin and liraglutide provides superior protection against diabetes-induced cardiorenal injury compared to either treatment alone, highlighting their potential as adjunctive therapies in reducing type 2 diabetes mellitus complications.
Keywords: cardio-renal injuries; dapagliflozin; liraglutide.
© 2025 Albanna et al.
Conflict of interest statement
The authors declare that they have no competing interests in this work.
Figures











Similar articles
-
Study on the modulation of kidney and liver function of rats with diabetic nephropathy by Huidouba through metabolomics.J Ethnopharmacol. 2025 Jul 24;351:120136. doi: 10.1016/j.jep.2025.120136. Epub 2025 Jun 11. J Ethnopharmacol. 2025. PMID: 40513925
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Dipeptidyl-peptidase (DPP)-4 inhibitors and glucagon-like peptide (GLP)-1 analogues for prevention or delay of type 2 diabetes mellitus and its associated complications in people at increased risk for the development of type 2 diabetes mellitus.Cochrane Database Syst Rev. 2017 May 10;5(5):CD012204. doi: 10.1002/14651858.CD012204.pub2. Cochrane Database Syst Rev. 2017. PMID: 28489279 Free PMC article.
-
Genistein Enhances the Beneficial Effects of Exercise on Antioxidant and Anti-inflammatory Balance and Cardiomyopathy in Ovariectomized Diabetic Rats.Antiinflamm Antiallergy Agents Med Chem. 2025;24(2):103-113. doi: 10.2174/0118715230305886240916105248. Antiinflamm Antiallergy Agents Med Chem. 2025. PMID: 39482917
-
Sertindole for schizophrenia.Cochrane Database Syst Rev. 2005 Jul 20;2005(3):CD001715. doi: 10.1002/14651858.CD001715.pub2. Cochrane Database Syst Rev. 2005. PMID: 16034864 Free PMC article.
References
-
- Federation I. IDF Diabetes Atlas, tenth. International Diabetes. 2021.
LinkOut - more resources
Full Text Sources
Miscellaneous
