

Management of Pancreatectomy for Pancreatic Cancer in a Patient With Annular Portal Pancreas: A Case Report
- PMID: 40656240
- PMCID: PMC12256133
- DOI: 10.7759/cureus.85950
Management of Pancreatectomy for Pancreatic Cancer in a Patient With Annular Portal Pancreas: A Case Report
Abstract
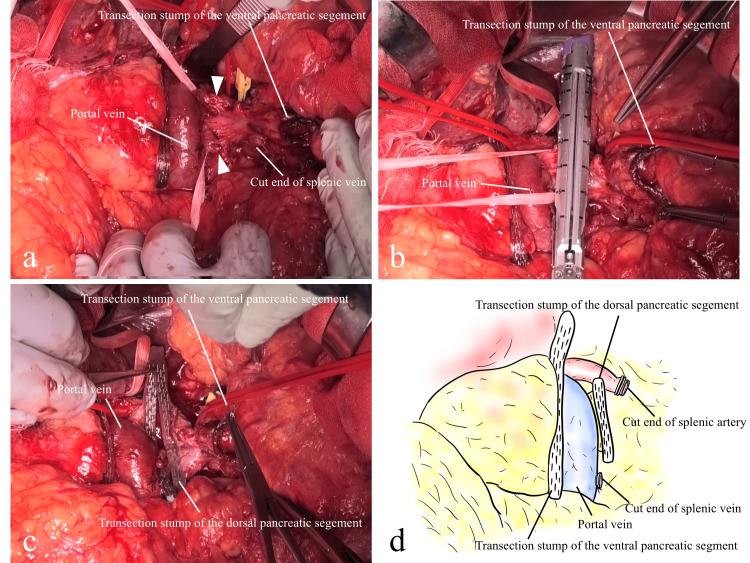
Portal annular pancreas (PAP) is one of the rare pancreatic anomalies in which the pancreatic parenchyma surrounds the portal vein (PV) or superior mesenteric vein (SMV), accounting for only around a few proportions of all patients. PAP is thought to be associated with the high risk of postoperative pancreatic fistula (POPF) after pancreatectomy. We describe our experience of a case with PAP and review the literature on pancreatectomy in patients with PAP. A 72-year-old male presented to our department with a pancreatic body mass with a history of previous abdominal surgeries, who underwent distal pancreatectomy (DP) with lymphadenectomy following neoadjuvant chemotherapy with gemcitabine plus nab-paclitaxel. PAP was identified during surgery, which was not found in computed tomography scans and other modalities in the previous examinations. The annular pancreas was resected using tri-staplers with polyglycolic acid (PGA) sheets. His postoperative course was uneventful without POPF, and he was discharged on postoperative day 11. In conclusion, when PAP is suspected in patients with pancreatic cancer, understanding the accurate anatomy of the pancreas is essential to determine the surgical technique and a suitable choice of device for the transection of pancreatic parenchyma for reducing POPF.
Keywords: pancreatic abnormality; pancreatic fistula; pancreatic malformation; rare variation; surgical complication.
Copyright © 2025, Hakoda et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures


References
-
- Portal annular pancreas. A rare variant and a new classification. Joseph P, Raju RS, Vyas FL, Eapen A, Sitaram V. https://pubmed.ncbi.nlm.nih.gov/20818114/ JOP. 2010;11:453–455. - PubMed
-
- The hypertrophic uncinate process of the pancreas wrapping the superior mesenteric vein and artery--a case report. Sugiura Y, Shima S, Yonekawa H, Yoshizumi Y, Ohtsuka H, Ogata T. Jpn J Surg. 1987;17:182–185. - PubMed
-
- Two cases of portal annular pancreas. Jang JY, Chung YE, Kang CM, Choi SH, Hwang HK, Lee WJ. Korean J Gastroenterol. 2012;60:52–55. - PubMed
-
- An extremely rare portal annular pancreas for pancreaticoduodenectomy with a special note on the pancreatic duct management in the dorsal pancreas. Matsumoto I, Shinzeki M, Fukumoto T, Ku Y. Surgery. 2013;153:434–436. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials