

Comparative Effectiveness of Robotic-Assisted, Video-Assisted, and Open Thymectomy for Thymoma: A Systematic Review and Meta-Analysis
- PMID: 40656279
- PMCID: PMC12254026
- DOI: 10.7759/cureus.85806
Comparative Effectiveness of Robotic-Assisted, Video-Assisted, and Open Thymectomy for Thymoma: A Systematic Review and Meta-Analysis
Abstract
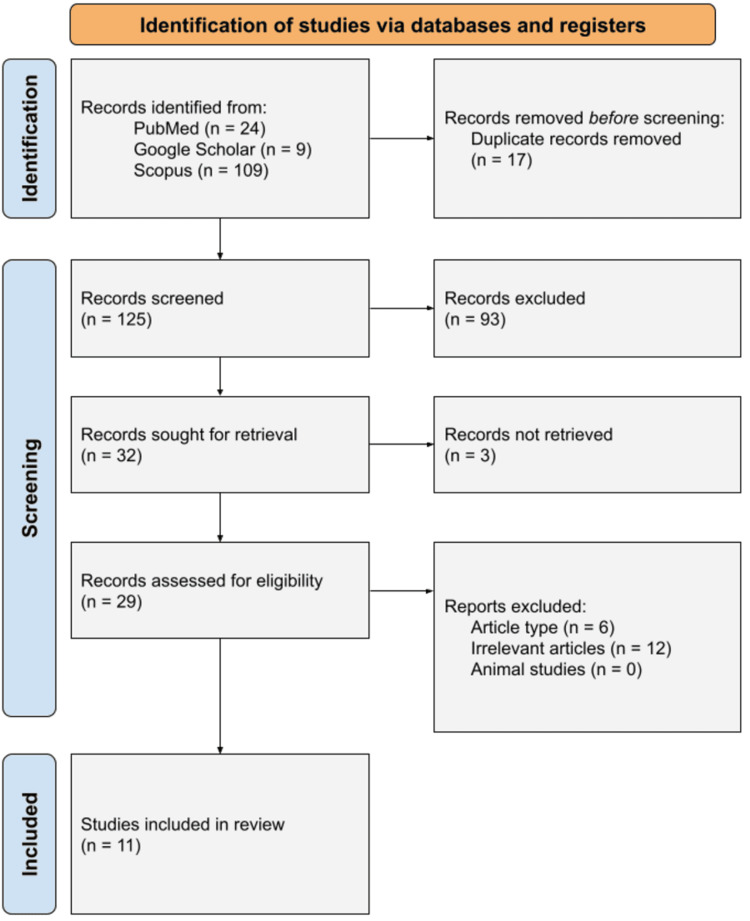
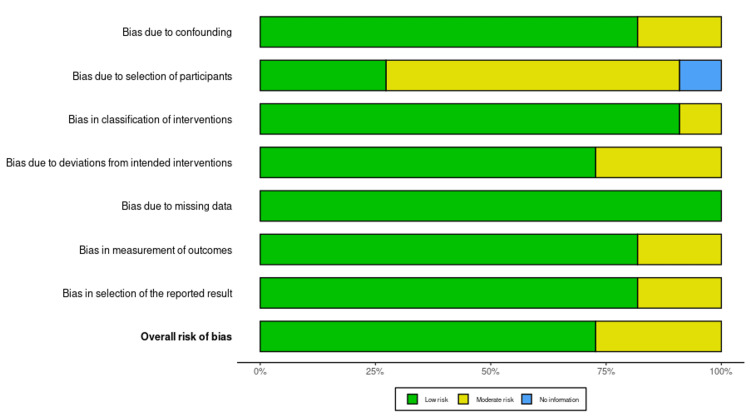
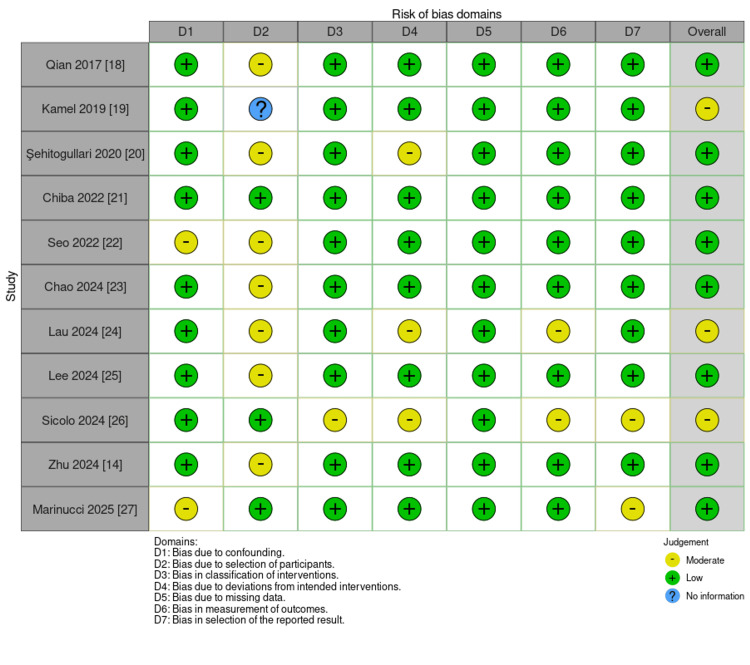
Thymoma is the most common primary mediastinal tumor in adults, typically excised in a single operation. Less invasive approaches, specifically robotic-assisted thymectomy surgery (RATS) and video-assisted thoracoscopic surgery (VATS), have gained popularity subsequent to conventional open thymectomy via median sternotomy. To determine the best surgery for thymoma, this systematic review and meta-analysis compared RATS, VATS, and total thymectomy in terms of efficacy, safety, and prognosis. Literature databases were systematically reviewed for publications, including PubMed, Scopus, and Google Scholar, till February 2025, using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) criteria sectioning the articles based on comparison of RATS to VATS or open thymectomy, as well as quantitative outcomes of reoperation, total survival, recurrence, perioperative complications, length of procedure, and length of stay. The risk of bias was assessed using the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool. Eleven articles met the eligibility criteria, and data were analyzed using random-effects model meta-analysis on RevMan (Cochrane, London, UK). RATS had comparable operation times to VATS (pooled mean difference: 4.49 minutes; 95% CI: -39.87 to 48.84; I² = 98%); it was, however, linked with fewer total complications (mean difference: -3.78; 95% CI: -3.89 to -3.70) and less intraoperative blood loss (mean difference: -25.01 mL; 95% CI: -38.03 to -12.00; I² = 0%). Also, RATS showed a reduction in pleural drainage time compared to VATS (mean difference: -0.66 days; 95% CI: -0.97 to -0.35; I² = 0%). RATS led to shorter hospital stays than open thymectomy (mean difference versus VATS: -0.28 days; 95% CI: -1.36 to 0.80; I² = 91%; versus open: -1.38 days; 95% CI: -2.33 to -0.43; I² = 14%) and fewer postoperative complications than open thymectomy but not differences in oncologic outcomes, including mortality and rates of recurrence. The I² values ranged widely from 0% to 98%, indicating variable heterogeneity across outcomes, which limits interpretability in some comparisons. Most studies included were retrospective cohorts, and the risk of bias was inconsistent, with one study deemed to be at low risk and seven deemed to have some concerns. Overall heterogeneity between outcomes ranged from low to moderate (I² = 0%-98%). Issues with costs and surgeon experience variability, however, continue to be major impediments to routine use of RATS. Given the retrospective nature of most included studies and high heterogeneity in key outcomes, conclusions about RATS's comparative advantage should be interpreted cautiously. While RATS demonstrates similar oncologic outcomes with fewer complications and shorter hospital stays, its routine use remains constrained by cost, surgeon training requirements, and a lack of high-quality prospective data. Future multicenter randomized controlled trials and cost-effectiveness studies are necessary to clarify its long-term role in thymoma surgery.
Keywords: open thymectomy; robotic; robotic-assisted thoracoscopic surgery (rats); thymectomy; video-assisted thoracoscopic surgery (vats).
Copyright © 2025, La et al.
Conflict of interest statement
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures







Similar articles
-
Does Minimally Invasive Surgery Provide Better Clinical or Radiographic Outcomes Than Open Surgery in the Treatment of Hallux Valgus Deformity? A Systematic Review and Meta-analysis.Clin Orthop Relat Res. 2023 Jun 1;481(6):1143-1155. doi: 10.1097/CORR.0000000000002471. Epub 2022 Nov 4. Clin Orthop Relat Res. 2023. PMID: 36332131 Free PMC article.
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Pre-operative endometrial thinning agents before endometrial destruction for heavy menstrual bleeding.Cochrane Database Syst Rev. 2013 Nov 15;2013(11):CD010241. doi: 10.1002/14651858.CD010241.pub2. Cochrane Database Syst Rev. 2013. PMID: 24234875 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
References
-
- Primary mediastinal tumors. Part 1: tumors of the anterior mediastinum. Strollo DC, Rosado de Christenson ML, Jett JR. Chest. 1997;112:511–522. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous