

Source control in bloodstream infections in patients with sepsis, septic shock, or requiring ICU admission: a scoping review with recommendations for standardizing research
- PMID: 40658248
- PMCID: PMC12317914
- DOI: 10.1007/s00134-025-08026-5
Source control in bloodstream infections in patients with sepsis, septic shock, or requiring ICU admission: a scoping review with recommendations for standardizing research
Abstract
Background: Bloodstream infections (BSI) account for 15% of intensive care unit (ICU) infections, often causing sepsis with mortality rates up to 50%. Source control (SC), encompassing interventions to reduce bacterial or fungal load and prevent infection spread, is a critical yet under-investigated component of management.
Objectives: This scoping review examines SC definitions, interventions, timing, adequacy, and outcomes in BSI literature in patients with sepsis, septic shock, or ICU admission, and offers a proposal for standardized reporting.
Methods: We searched Medline, EMBASE, and Cochrane Library for studies on adult BSI addressing SC in populations with ≥ 50% ICU admission, ≥ 75% sepsis, or ≥ 25% septic shock, extracted and reported data following established guidance.
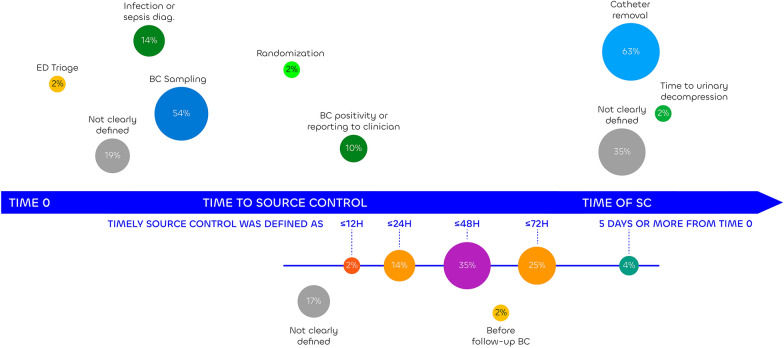
Results: From 2193 abstracts, 77 studies were included. SC was a primary objective in 21%, with others reporting it alongside other objectives. Candidemia (47%) and catheter removal (60%) studies were predominant, with 34% evaluating catheter removal regardless of BSI source. SC definitions varied from no definition (8%), minimal (7%), concise (17%), comprehensive (9%) definitions and catheter removal (60%). Forty-seven % reported proportions receiving SC for the entire cohort rather than those requiring SC. Timing was reported by 68%, with inconsistent definitions. SC adequacy was assessed by 3%. SC improved outcomes in 65%, with no reported harm.
Conclusion: SC research in severe BSI is limited by inconsistent definitions, poor SC efficacy assessments, and overrepresentation of catheter-source BSI and candidemia. Standardized reporting is essential to enhance evidence quality and optimize BSI management in critically ill patients.
Keywords: Bloodstream infection; Sepsis; Source; Source control.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflicts of interest: Alexis Tabah has nothing to disclose, Jan De Waele has consulted for Biomerieux, Menarini, MSD, Pfizer, Roche Diagnostics, ThermoFisher and Viatris (fees and honoraria paid to institution), Nathalie Ssi Yan Kai has nothing to disclose, Abdullah Tarik Aslan has nothing to disclose, Niccolo Buetti has nothing to disclose, Jean-François Timsit reported advisory boards participation for Merck, Gilead, Beckton-Dickinson, Pfizer, Menarini, Advanz, Paratek, research grants from Merck and Pfizer, Emma Ballard has nothing to disclose, Lars Eriksson, Kevin Laupland reported grants to his research unit from Pfizer and Merck, consulting fees from Menarini, Merck, Biomerieux, Roche diagnostics advanz, all outside of the submitted work, lecture honoraria from Pfizer, Merck, Biomerieux, Shionogi, advanz, Gilead mundipharma outside of the submitted work, and support for attending meetings from Tillots. Jeffrey Lipman has nothing to disclose. Jan De Waele is supported by a Sr Clinical Research Grant from the Research Foundation Flanders (FWO, Ref. 1881020N). Ethical approval: Since our scoping review did not involve human or animal studies, no ethics committee approval was required, and the study adheres to the ethical standards outlined in the 1964 Declaration of Helsinki and its later amendments.
Figures
Similar articles
-
Systemic Inflammatory Response Syndrome.2025 Jun 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jun 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 31613449 Free Books & Documents.
-
Automated monitoring compared to standard care for the early detection of sepsis in critically ill patients.Cochrane Database Syst Rev. 2018 Jun 25;6(6):CD012404. doi: 10.1002/14651858.CD012404.pub2. Cochrane Database Syst Rev. 2018. PMID: 29938790 Free PMC article.
-
High-volume haemofiltration for sepsis in adults.Cochrane Database Syst Rev. 2017 Jan 31;1(1):CD008075. doi: 10.1002/14651858.CD008075.pub3. Cochrane Database Syst Rev. 2017. PMID: 28141912 Free PMC article.
-
Glutamine supplementation for critically ill adults.Cochrane Database Syst Rev. 2014 Sep 9;2014(9):CD010050. doi: 10.1002/14651858.CD010050.pub2. Cochrane Database Syst Rev. 2014. PMID: 25199493 Free PMC article.
-
Single induction dose of etomidate versus other induction agents for endotracheal intubation in critically ill patients.Cochrane Database Syst Rev. 2015 Jan 8;1(1):CD010225. doi: 10.1002/14651858.CD010225.pub2. Cochrane Database Syst Rev. 2015. PMID: 25568981 Free PMC article.
References
-
- Lee SY, Park MH, Oh DK, Lim CM, Korean Sepsis Alliance I (2024) Polymicrobial bloodstream infections per se do not increase mortality compared to monomicrobial bloodstream infections in sepsis patients: a Korean nationwide sepsis cohort study. BMC Infect Dis. 10.1186/s12879-024-09130-5 - PMC - PubMed
-
- Stewart AG, Laupland KB, Tabah A (2023) Central line associated and primary bloodstream infections. Curr Opin Crit Care 29(5):423–429. 10.1097/MCC.0000000000001082 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
