

Association of urinary dysfunction after lower rectal cancer surgery with renal function: a single-center study
- PMID: 40658254
- PMCID: PMC12259756
- DOI: 10.1007/s00384-025-04955-1
Association of urinary dysfunction after lower rectal cancer surgery with renal function: a single-center study
Abstract
Purpose: Urinary dysfunction (UD) is still a major complication after lower rectal cancer (LRC) surgery. Untreated UD is an independent risk factor for renal dysfunction due to repeated urinary reflux and urinary tract infections. However, the relationship between postoperative UD and renal function following LRC surgery remains unclear. In this study, we investigated the impact of UD on renal function post-surgery.
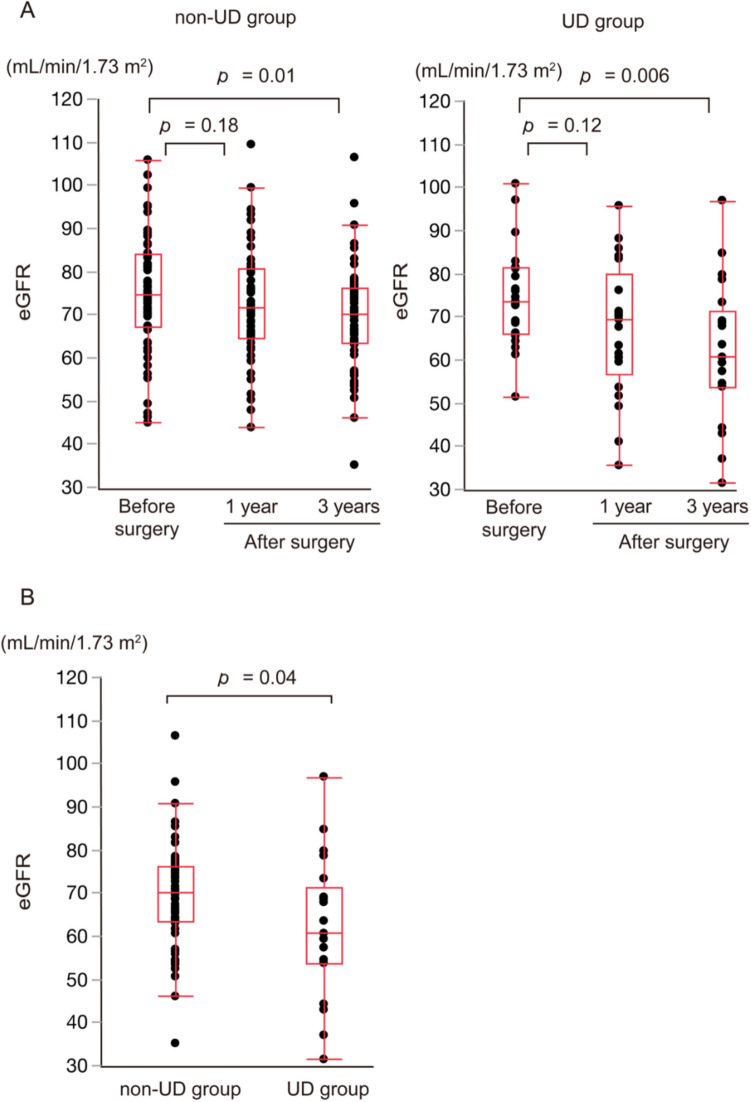
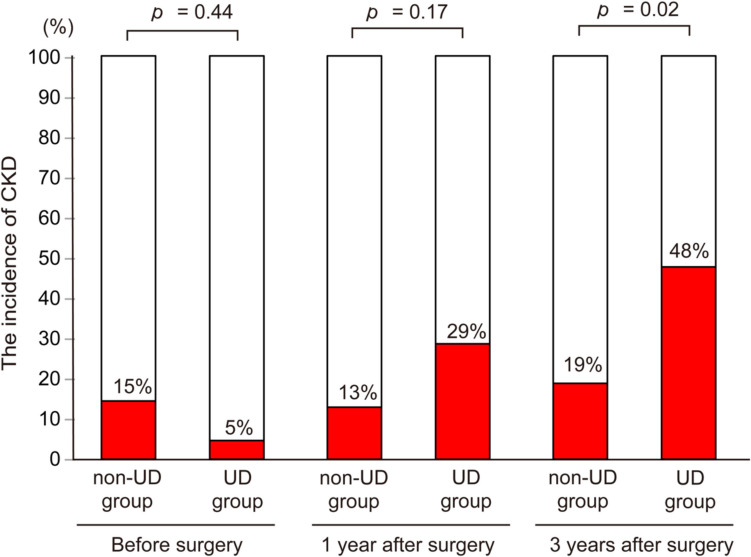
Methods: We retrospectively evaluated 83 patients with LRC who underwent curative resection at our tertiary referral center between April 2015 and December 2018. UD was diagnosed as a post-void residual urine volume ≥ 50 mL using uroflowmetry tests after discharge. We compared the estimated glomerular filtration rate (eGFR) and the incidence of chronic kidney disease (CKD)-defined as an eGFR < 60 mL/min/1.73 m2-at 3 years after LRC surgery between the UD and non-UD groups. Patient selection was based on the criteria that excluded those with a history of urogenital interventions or incomplete postoperative follow-up. Statistical analysis used the Mann-Whitney U test for continuous variables, Fisher's test for categorical data, and multivariate logistic regression to adjust for potential confounders.
Results: Of the 83 patients, 21 (25%) had UD. Patients with UD were older, underwent more extensive surgery, and had significantly longer operation times than those without UD. Within 3 years post-surgery, the UD group experienced a higher incidence of urinary tract complications and CKD, with a notable decrease in eGFR. Additionally, a history of hypertension and UD were identified as independent risk factors for CKD at 3 years post-surgery.
Conclusions: Patients with UD showed a significant decrease in eGFR and were more likely to progress to CKD at 3 years after LRC surgery. These findings indicated that postoperative UD might adversely affect renal function in patients with LRC.
Keywords: Lower rectal cancer; Postoperative renal dysfunction; Postoperative urinary dysfunction; Urinary tract complications; Uroflowmetry test.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: This study was performed in line with the principles of the Declaration of Helsinki and was conducted following approval from the Ethics Committee of the University of Tokyo Hospital (reference nos. 3252–16 and 10702-(7)). Consent to participate: Written informed consent was obtained from all the patients. Competing interests: The authors declare no competing interests.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
