

Crosstalk between lung and extrapulmonary organs in sepsis-related acute lung injury/acute respiratory distress syndrome
- PMID: 40658295
- PMCID: PMC12259525
- DOI: 10.1186/s13613-025-01513-4
Crosstalk between lung and extrapulmonary organs in sepsis-related acute lung injury/acute respiratory distress syndrome
Abstract
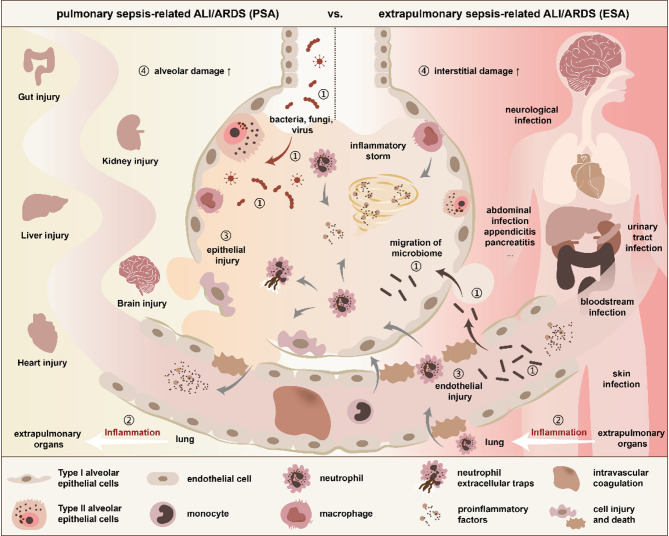
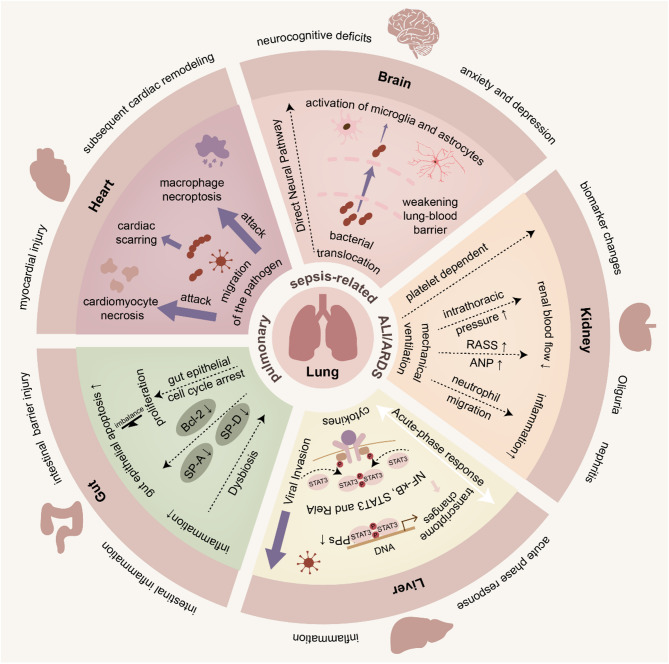
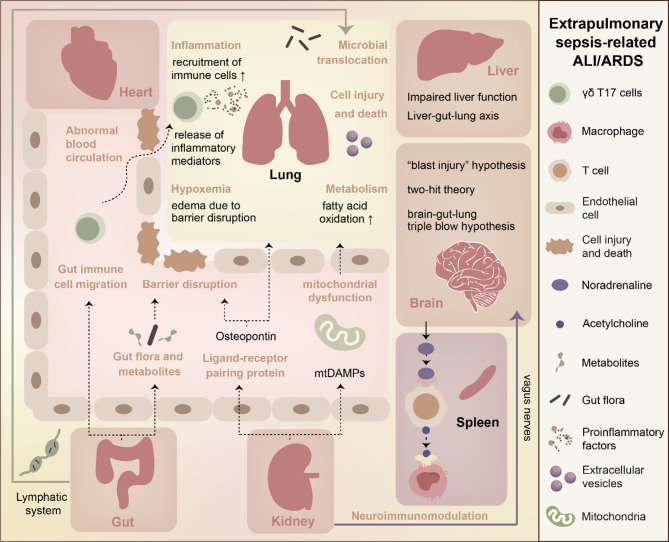
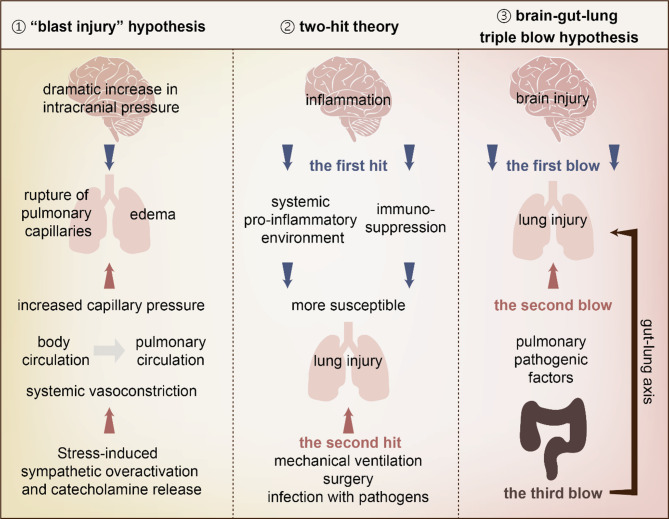
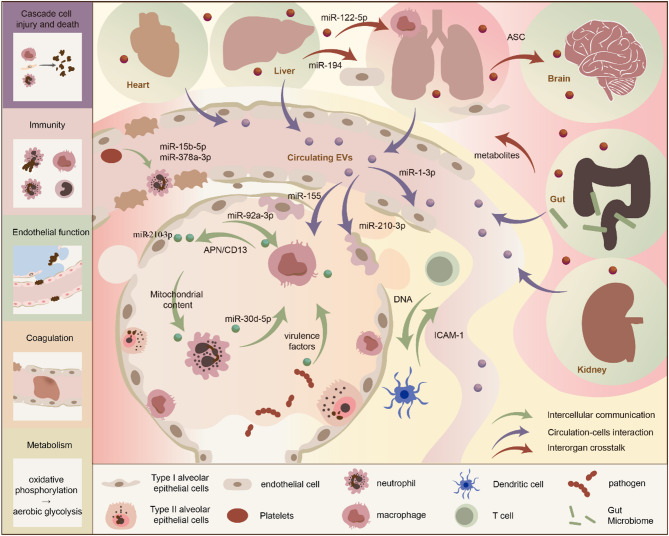
Sepsis-related acute lung injury/acute respiratory distress syndrome (ALI/ARDS) is associated with considerable morbidity and mortality, yet the efficacy of current treatments is limited. Previous studies have predominantly focused on the lung itself as an isolated organ, whereas the role of organ crosstalk in the pathogenesis of sepsis-related ALI/ARDS cannot be overlooked. Meanwhile, neglecting the discussion of heterogeneity in sepsis caused by different sources of infection may be another important obstacle to translating previous studies into clinical efficacy. In this review, we initially delineated the distinctions in pathogenesis between pulmonary and extrapulmonary sepsis-related ALI/ARDS in microbial species, pathogenesis, host response, and clinical manifestations. Additionally, systemic organ crosstalk mechanisms are summarized, including the commonality and specificity of systemic inflammation, lung and gut microbiome, as well as cascade cell injury and death in distant organs. Subsequently, organ crosstalk between lung and extrapulmonary in pulmonary sepsis and extrapulmonary sepsis-related ALI/ARDS are discussed by organs, including immunity, neuroendocrine, metabolism, and so forth. Furthermore, extracellular vesicles represent a promising avenue of research as potential players and targets in organ-lung crosstalk in sepsis. While the complexity of multi-organ interactions and the heterogeneity of septic patients present significant challenges, these issues are expected to be addressed by the emergence of organ-on-a-chip platforms, 3D organoid cultures, and multi-omics techniques.
Keywords: ALI/ARDS; Extracellular vesicles; Organ crosstalk; Sepsis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests.
Figures
Similar articles
-
Systemic Inflammatory Response Syndrome.2025 Jun 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jun 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 31613449 Free Books & Documents.
-
Pressure-controlled versus volume-controlled ventilation for acute respiratory failure due to acute lung injury (ALI) or acute respiratory distress syndrome (ARDS).Cochrane Database Syst Rev. 2015 Jan 14;1(1):CD008807. doi: 10.1002/14651858.CD008807.pub2. Cochrane Database Syst Rev. 2015. PMID: 25586462 Free PMC article.
-
Positioning for acute respiratory distress in hospitalised infants and children.Cochrane Database Syst Rev. 2022 Jun 6;6(6):CD003645. doi: 10.1002/14651858.CD003645.pub4. Cochrane Database Syst Rev. 2022. PMID: 35661343 Free PMC article.
-
Pulmonary coagulopathy as a new target in lung injury--a review of available pre-clinical models.Curr Med Chem. 2008;15(6):588-95. doi: 10.2174/092986708783769696. Curr Med Chem. 2008. PMID: 18336273
-
Partial liquid ventilation for preventing death and morbidity in adults with acute lung injury and acute respiratory distress syndrome.Cochrane Database Syst Rev. 2013 Jul 23;2013(7):CD003707. doi: 10.1002/14651858.CD003707.pub3. Cochrane Database Syst Rev. 2013. PMID: 23881653 Free PMC article.
References
-
- Wick KD, Ware LB, Matthay MA. Acute respiratory distress syndrome. BMJ (Clinical research ed.). 2024;387:e076612. - PubMed
-
- Lelubre C, Vincent J. Mechanisms and treatment of organ failure in sepsis. Nat Rev Nephrol. 2018;14(7):417–27. - PubMed
-
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, et al. Surviving Sepsis campaign: international guidelines for management of Sepsis and septic shock: 2016. Intensive Care Med. 2017;43(3):304–77. - PubMed
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315(8):788–800. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
