

Geographic variation in utilization of deceased donor livers in the United States in the era of advanced perfusion
- PMID: 40658771
- PMCID: PMC12327723
- DOI: 10.1097/LVT.0000000000000687
Geographic variation in utilization of deceased donor livers in the United States in the era of advanced perfusion
Abstract
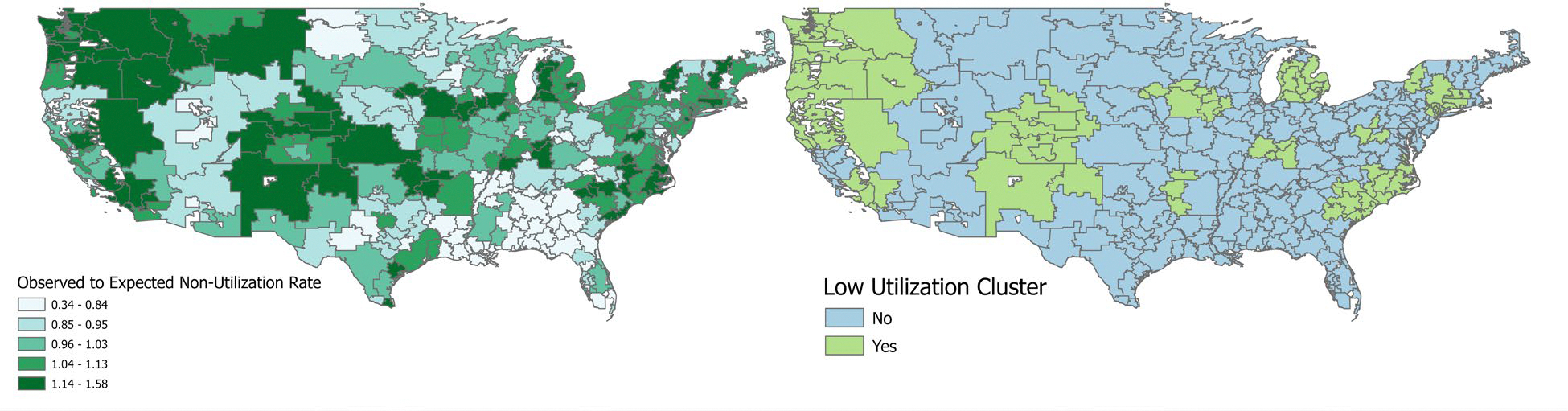
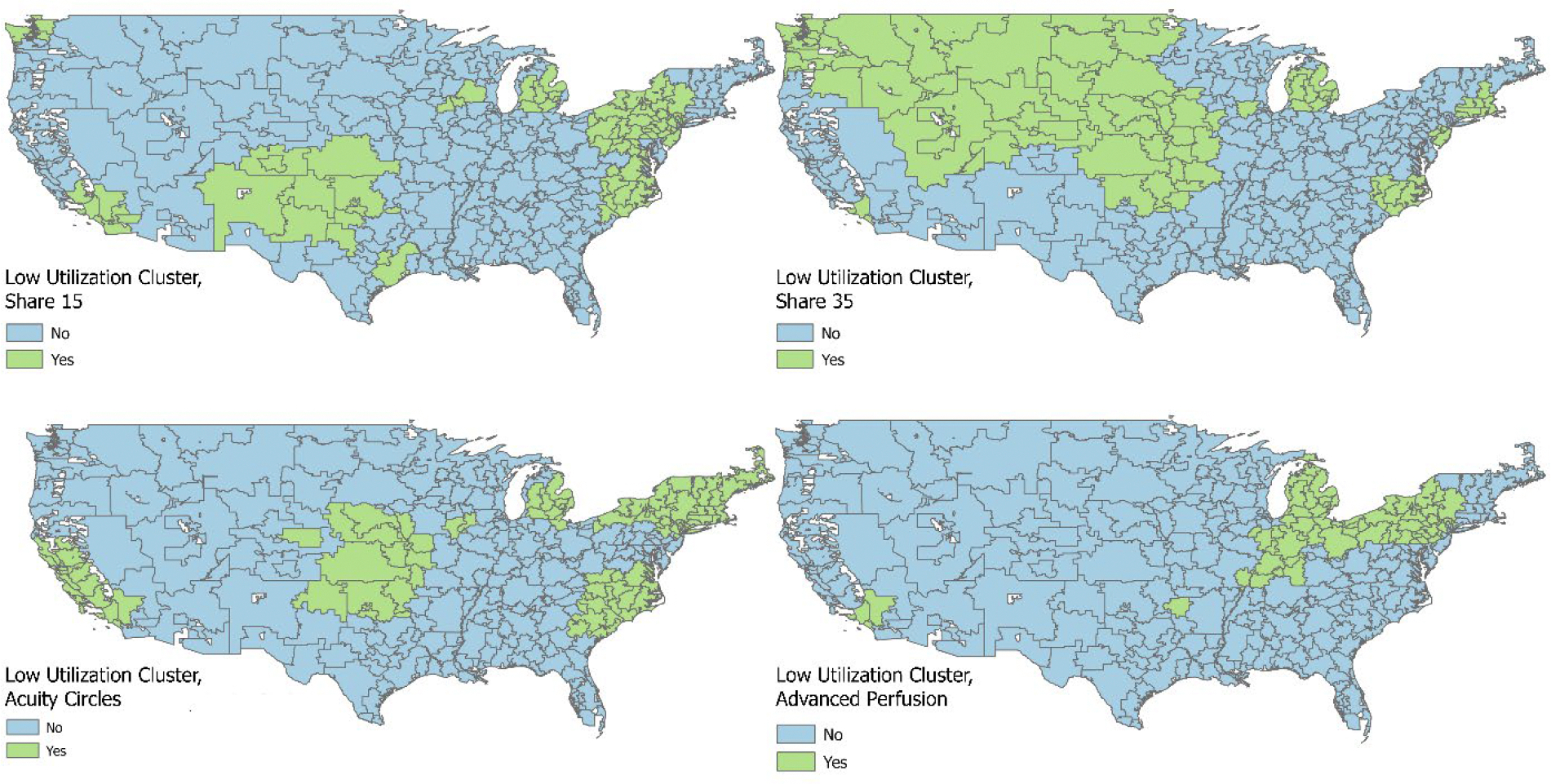
Understanding the geographic variation in deceased donor liver utilization can guide allocation policy and technology implementation. Using US transplant registry data, we evaluated geographic differences in utilization by donor quality, policy era, and uptake of advanced perfusion (AP). This retrospective cohort included all liver donors and waitlisted patients from 2010 to September 2024. Donors were aggregated by Hospital Referral Region (HRR) and stratified by quality using the liver Discard Risk Index (DSRI). Exposures included the allocation policy era and increased use of AP technology (July 2022 onward). Observed-to-expected (O:E) ratios of liver non-utilization were calculated by HRR and modeled to reveal geographically contiguous low utilization clusters (LUCs). The proportion of HRRs within LUCs increased from 24% in Share 15 (S15), to 25% in Share 35 (S35), 32% in Acuity Circles (AC), and then decreased to 21% in the AP era ( p =0.01). There were 7 distinct LUCs in S15 (median non-utilization=33%), 7 LUCs in S35 (non-utilization=32%), 7 LUCs in AC (non-utilization=41%), and 3 LUCs in the AP era (non-utilization=46%). Donor quality by HRR decreased over time, with a median DSRI of 2.56 (IQR: 1.25-5.79) in S15 to 5.69 (2.01-35.30) in AP ( p <0.001). Accounting for DSRI, odds of non-utilization were highest in AC ( ref. Share 35 , OR=1.27, p <0.001), which decreased in AP (OR=1.06, p =0.001). Utilization of normothermic machine perfusion was associated with a markedly lower odds of discard (OR=0.03, 0.03-0.04; p <0.001). Livers originating from LUCs traveled shorter distances in each era other than S35. The number of net exporter HRRs in LUCs was equivalent to non-LUCs in each era, other than AP, where LUCs contained fewer net exporter HRRs [2 (3.2%) vs. 42 (17.4%), p =0.004]. On adjusted analysis, candidates in LUCs had a lower likelihood of transplant (HR=0.88, p <0.001) but also lower waitlist mortality (HR=0.95, p <0.001). The advent of advanced perfusion was associated with the utilization of otherwise marginal liver allografts and ameliorating geographic imbalances in discard seen with successive allocation policy eras.
Keywords: advanced perfusion; allocation policy; normothermic machine perfusion; organ procurement organizations; organ utilization.
Copyright © 2025 American Association for the Study of Liver Diseases.
Conflict of interest statement
Figures
References
-
- Ahearn A The history of ethical principles in liver transplant organ allocation in the United States: how historical and proposed allocations system fare in balancing utility vs. urgency and justice vs. pragmatism. Curr Opin Organ Transplant. 2023;28(6):452–456. doi: 10.1097/MOT.0000000000001103 - DOI - PubMed
-
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Health Care Services; Board on Health Sciences Policy; Committee on A Fairer and More Equitable, Cost-Effective, and Transparent System of Donor Organ Procurement, Allocation, and Distribution. Realizing the Promise of Equity in the Organ Transplantation System. (Hackmann M, English RA, Kizer KW, eds.). National Academies Press; (US: ); 2022. Accessed February 28, 2025. http://www.ncbi.nlm.nih.gov/books/NBK578320/ - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
