

Performance of Natural Language Processing versus International Classification of Diseases Codes in Building Registries for Patients With Fall Injury: Retrospective Analysis
- PMID: 40658984
- PMCID: PMC12279314
- DOI: 10.2196/66973
Performance of Natural Language Processing versus International Classification of Diseases Codes in Building Registries for Patients With Fall Injury: Retrospective Analysis
Abstract
Background: Standardized registries, such as the International Classification of Diseases (ICD) codes, are commonly built using administrative codes assigned to patient encounters. However, patients with fall injury are often coded using subsequent injury codes, such as hip fractures. This necessitates manual screening to ensure the accuracy of data registries.
Objective: This study aimed to automate the extraction of fall incidents and mechanisms using natural language processing (NLP) and compare this approach with the ICD method.
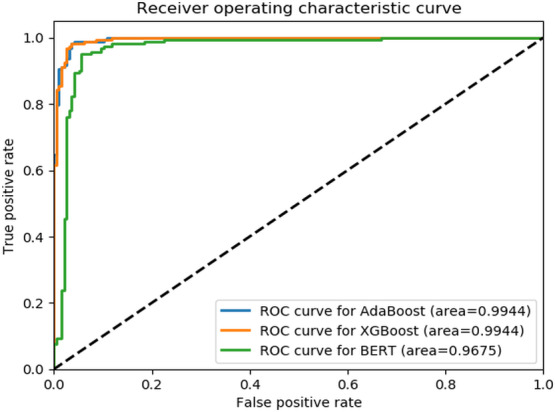
Methods: Clinical notes for patients with fall-induced hip fractures were retrospectively reviewed by medical experts. Fall incidences were detected, annotated, and classified among patients who had a fall-induced hip fracture (case group). The control group included patients with hip fractures without any evidence of falls. NLP models were developed using the annotated notes of the study groups to fulfill two separate tasks: fall occurrence detection and fall mechanism classification. The performances of the models were compared using accuracy, sensitivity, specificity, positive predictive value, negative predictive value, F1-score, and area under the receiver operating characteristic curve.
Results: A total of 1769 clinical notes were included in the final analysis for the fall occurrence task, and 783 clinical notes were analyzed for the fall mechanism classification task. The highest F1-score using NLP for fall occurrence was 0.97 (specificity=0.96; sensitivity=0.97), and for fall mechanism classification was 0.61 (specificity=0.56; sensitivity=0.62). Natural language processing could detect up to 98% of the fall occurrences and 65% of the fall mechanisms accurately, compared to 26% and 12%, respectively, by ICD codes.
Conclusions: Our findings showed promising performance with higher accuracy of NLP algorithms compared to the conventional method for detecting fall occurrence and mechanism in developing disease registries using clinical notes. Our approach can be introduced to other registries that are based on large data and are in need of accurate annotation and classification.
Keywords: AI; ICD Codes; LLMs; ML; NLP; algorithms; artificial intelligence; automate; automation; data registry; deep learning; large language models; machine learning; natural language processing; predictive analytics; predictive models.
© Atta Taseh, Souri Sasanfar, Michelle Chan, Evan Sirls, Ara Nazarian, Kayhan Batmanghelich, Jonathan F Bean, Soheil Ashkani-Esfahani. Originally published in JMIR Medical Informatics (https://medinform.jmir.org).
Conflict of interest statement
Figures


References
-
- Cost of older adult falls. US Centers for Disease Control and Prevention. [17-07-2024]. https://stacks.cdc.gov/view/cdc/122747 URL. Accessed.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
