

Colchicine in patients with aortic stenosis undergoing transcatheter aortic valve replacement: a double-blind randomized trial
- PMID: 40659682
- PMCID: PMC12259991
- DOI: 10.1038/s41467-025-61916-6
Colchicine in patients with aortic stenosis undergoing transcatheter aortic valve replacement: a double-blind randomized trial
Abstract
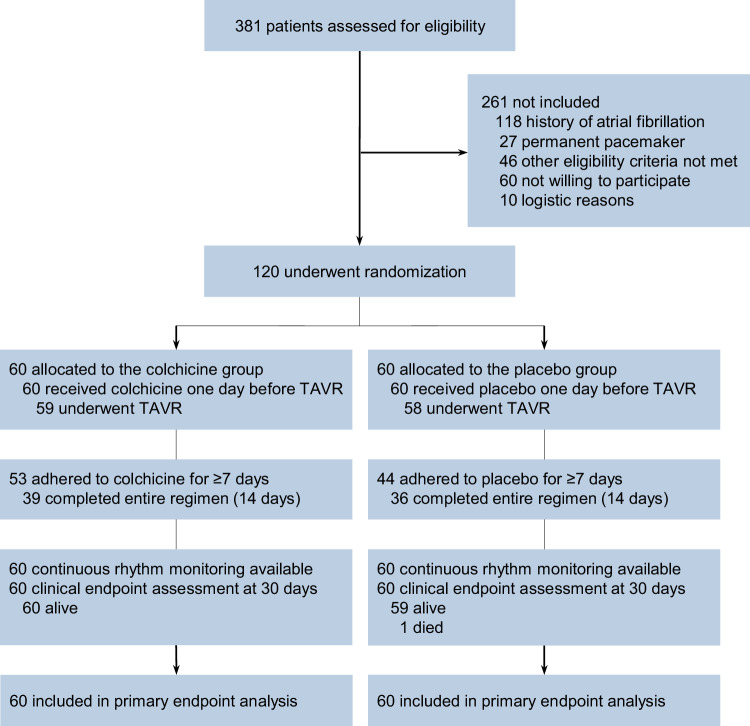
An inflammatory process may increase the risk of arrhythmias after transcatheter aortic valve replacement (TAVR). In this single-centre, double-blind, placebo-controlled, randomized trial we investigated the efficacy of colchicine to reduce a composite of new-onset atrial fibrillation or atrioventricular conduction disturbances requiring the implantation of a permanent pacemaker at 30 days after TAVR. Between September 21, 2021 and April 25, 2024, 120 patients with aortic stenosis undergoing TAVR (mean age 80.6 ± 5 years, 64% male) were randomly allocated to treatment with colchicine (n = 60) or placebo (n = 60). The trial was prematurely stopped due to a higher rate of stroke in the experimental group in a pre-specified interim analysis (5 [8.3%] versus 0 at maximum available follow-up, p = 0.022). In the intention-to-treat population, the primary endpoint occurred in 6 patients (10%) in the colchicine group and in 15 patients (25%) in the placebo group (risk-difference -15.0%, 95% CI -28.3 to -1.7, p = 0.031). The prespecified imaging endpoint, subclinical leaflet thrombosis, was detected in 13 of 48 patients (27%) in the colchicine group versus 26 of 48 patients (54%) in the placebo group (risk difference -27.1%. 95% CI -46.0% to -8.2%, p = 0.007). Here, we show that periprocedural treatment with colchicine may reduce the incidence of new-onset arrhythmias and subclinical leaflet thrombosis after TAVR. However, given the premature termination of the trial due to an unexpected increase in the stroke rate among patients treated with colchicine, confirmatory trials are warranted to corroborate the effect of anti-inflammatory treatment on the incidence of arrhythmias and subclinical leaflet thrombosis after TAVR. The trial was an investigator-initiated study supported by dedicated grants from the Bangerter-Rhyner Foundation and the Swiss Life Foundation. ClinicalTrials.gov Identifier: NCT04870424.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: Jonas Lanz reports speaker fees from Edwards Lifesciences and Abbott to the institution. Daryoush Samim has received funding for an online course from Edwards Lifesciences. Stefan Stortecky reports research grants to the institution from Edwards Lifesciences, Medtronic, Abbott, Boston Scientific, and consultancy fees from BTG / Boston Scientific, and Teleflex outside the submitted work. Dik Heg is employed by the DCR, University of Bern, which has a staff policy of not accepting honoraria or consultancy fees. However, DCR is involved in design, conduct, or analysis of clinical studies funded by not-for-profit and for-profit organizations. In particular, pharmaceutical and medical device companies provide direct funding to some of these studies. For an up-to-date list of our conflicts of interest see https://www.ctu.unibe.ch/research_projects/declaration_of_interest/index_eng.html . David Reineke reports travel expenses from Abbott, Edwards Lifesciences and Medtronic and has proctor and consulting contracts with Abbott and Medtronic. Tobias Reichlin: Research grants from the Swiss National Science Foundation, the Swiss Heart Foundation, the sitem insel support funds, Biotronik, Boston Scientific and Medtronic, all for work outside the submitted study. Speaker/consulting honoraria or travel support from Abbott/SJM, Bayer, Biosense-Webster, Biotronik, Boston-Scientific, Farapulse, Medtronic, Pfizer-BMS, all for work outside the submitted study. Support for his institution’s fellowship program from Abbott/SJM, Biosense-Webster, Biotronik, Boston-Scientific and Medtronic for work outside the submitted study. Christoph Gräni has received funding support from the Swiss National Science Foundation, InnoSuisse, the CAIM foundation, the GAMBIT foundation, and the Novartis Biomedical Research Foundation. Stephan Windecker reports research, travel or educational grants to the institution from Abbott, Abiomed, Amgen, Astra Zeneca, Bayer, Bbraun, Biotronik, Boehringer Ingelheim, Boston Scientific, Bristol Myers Squibb, Cardinal Health, CardioValve, Cleerly Inc., Cordis Medical, Corflow Therapeutics, CSL Behring, Daiichi Sankyo, Edwards Lifesciences, Farapulse Inc. Fumedica, GE Medical Systems, Gebro Pharma, Guerbet, Idorsia, Inari Medical, InfraRedx, Janssen-Cilag, Johnson & Johnson, Medalliance, Medicure, Medtronic, Merck Sharp & Dohm, Miracor Medical, Neucomed, Novartis, Novo Nordisk, Organon, OrPha Suisse, Pharming Tech, Pfizer, Philips AG, Polares, Regeneron, Sanofi-Aventis, Servier, Siemens Healthcare, Sinomed, SMT Sahajanand Medical Technologies, Terumo, Vifor, V-Wave, Zoll Medical. Stephan Windecker served as advisory board member and/or member of the steering/executive group of trials funded by Abbott, Abiomed, Amgen, Astra Zeneca, Bayer, Boston Scientific, Biotronik, Bristol Myers Squibb, Edwards Lifesciences, MedAlliance, Medtronic, Novartis, Polares, Recardio, Sinomed, Terumo, and V-Wave with payments to the institution but no personal payments. He is also member of the steering/executive committee group of several investigator-initiated trials that receive funding by industry without impact on his personal remuneration. Thomas Pilgrim reports research grants from the Swiss National Science Foundation, the Swiss Heart Foundation, the Swiss Polar Institute, the Bangerter-Rhyner Foundation, the Mach-Gaensslen Foundation, and the Monsol Foundation. Research, travel or educational grants to the institution without personal remuneration from Biotronik, Boston Scientific, Edwards Lifesciences, and ATSens; speaker fees and consultancy fees to the institution from Biotronik, Boston Scientific, Edwards Lifesciences, Abbott, Medtronic, Biosensors, and Highlife. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures



References
-
- Siontis, G. C. M. et al. Transcatheter aortic valve implantation vs. surgical aortic valve replacement for treatment of symptomatic severe aortic stenosis: an updated meta-analysis. Eur. Heart J.40, 3143–3153 (2019). - PubMed
-
- Pilgrim, T., Siontis, G. C. M. & Windecker, S. Transcatheter aortic valve implantation: a blueprint for evidence-based evaluation of technological innovation. Eur. Heart J.44, 853–855 (2023). - PubMed
-
- Ryan, T. et al. New-Onset Atrial Fibrillation After Transcatheter Aortic Valve Replacement: A Systematic Review and Meta-Analysis. JACC Cardiovasc. Interv.15, 603–613 (2022). - PubMed
-
- Bruno, F. et al. Predictors of pacemaker implantation after transcatheter aortic valve implantation according to kind of prosthesis and risk profile: a systematic review and contemporary meta-analysis. Eur. Heart J. Qual. Care Clin. Outcomes7, 143–153 (2021). - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
