

The use of deliberate practice in simulation-based surgical training for laparoscopic surgery - a systematic review
- PMID: 40660230
- PMCID: PMC12257738
- DOI: 10.1186/s12909-025-07613-w
The use of deliberate practice in simulation-based surgical training for laparoscopic surgery - a systematic review
Abstract
Background: Minimally Invasive Surgery (MIS) has necessitated specialized training beyond traditional open surgical methods. Simulation-Based Surgical Training (SBST) offers a promising alternative, but its instructional design varies significantly. Deliberate Practice (DP), a concept originating from expertise research, may enhance SBST effectiveness. This systematic review evaluates the integration of DP within SBST for MIS.
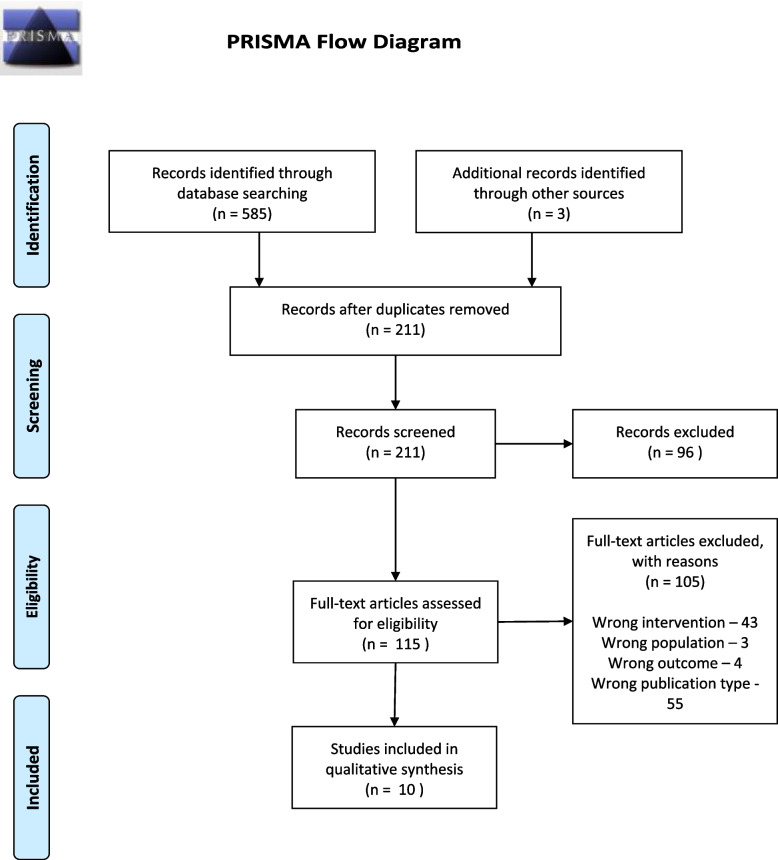
Methods: A systematic literature search was conducted using MEDLINE, EMBASE, SCOPUS, ERIC, and Google Scholar, covering publications up to January 31, 2024. Randomized controlled trials and observational studies implementing DP in SBST for laparoscopic surgery were included. Data extraction focused on DP elements (task design, feedback, and repetition), learner motivation, training structure, and outcome measures. Study quality and risk of bias were assessed using the RoB2 and ROBINS-E tools.
Results: Ten studies met inclusion criteria, comprising five randomized controlled trials and five observational studies. Study participants were predominantly surgical trainees, with training programs utilizing box trainers or virtual reality simulators. DP-informed SBST was consistently associated with improved psychomotor skills, particularly when feedback was immediate, and training incorporated structured task progression. Task design varied, with only two studies tailoring training based on pre-existing skill levels. Stepwise task progression was reported in five studies. Feedback was delivered through either human mentors or automated simulator feedback, with mixed findings on their comparative effectiveness. While automated feedback ensured immediacy, human supervision was often deemed superior in guiding skill acquisition. Repetition was widely integrated, though session duration and spacing varied across studies. Learner motivation was explicitly assessed in one study, while two others incorporated motivation-enhancing interventions such as gamification and mentoring. DP-informed SBST resulted in improved accuracy, speed, confidence, and objective skill ratings. Some control groups also demonstrated skill improvements, though typically reaching performance plateaus earlier and at lower competency levels. Variability in DP adherence across studies influenced outcomes, with the most structured programs yielding the greatest benefits.
Conclusions: DP-informed SBST is a promising approach for developing MIS skills. Adherence to DP principles significantly enhances skill acquisition but limited by resource requirements. Future research should focus on optimizing DP integration within SBST to maximize its impact on surgical education.
Keywords: Deliberate practice; Minimally invasive surgery; Simulation; Surgical training.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The need for ethics approval for systematic reviews has been waived off by the authors’ institution (Faculty of Medicine, University of Colombo, Sri Lanka). Ethics approval and consent to participate. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Health professionals' experience of teamwork education in acute hospital settings: a systematic review of qualitative literature.JBI Database System Rev Implement Rep. 2016 Apr;14(4):96-137. doi: 10.11124/JBISRIR-2016-1843. JBI Database System Rev Implement Rep. 2016. PMID: 27532314
-
Virtual reality training for improving the skills needed for performing surgery of the ear, nose or throat.Cochrane Database Syst Rev. 2015 Sep 9;2015(9):CD010198. doi: 10.1002/14651858.CD010198.pub2. Cochrane Database Syst Rev. 2015. PMID: 26352008 Free PMC article.
-
Virtual reality training for surgical trainees in laparoscopic surgery.Cochrane Database Syst Rev. 2013 Aug 27;2013(8):CD006575. doi: 10.1002/14651858.CD006575.pub3. Cochrane Database Syst Rev. 2013. PMID: 23980026 Free PMC article.
-
Interventions for interpersonal communication about end of life care between health practitioners and affected people.Cochrane Database Syst Rev. 2022 Jul 8;7(7):CD013116. doi: 10.1002/14651858.CD013116.pub2. Cochrane Database Syst Rev. 2022. PMID: 35802350 Free PMC article.
-
Parent training interventions for Attention Deficit Hyperactivity Disorder (ADHD) in children aged 5 to 18 years.Cochrane Database Syst Rev. 2011 Dec 7;2011(12):CD003018. doi: 10.1002/14651858.CD003018.pub3. Cochrane Database Syst Rev. 2011. PMID: 22161373 Free PMC article.
References
-
- Aghazadeh F, Fathian R, Zheng B, Tavakoli M, Rouhani H. Experts employ a target-locking behaviour in laparoscopic surgery. 2022.
-
- Stassen HG, Dankelman J, Grimbergen KA, Meijer DW. Man-machine aspects of minimally invasive surgery. Annu Rev Control. 2001;25:111–22.
-
- Bond WF, Lammers RL, Spillane LL, Smith-Coggins R, Fernandez R, Reznek MA, et al. The use of simulation in emergency medicine: a research agenda. Acad Emerg Med. 2007;14(4):353–63. - PubMed
-
- Singh H, Thomas EJ, Petersen LA, Studdert DM. Medical errors involving trainees. Arch Intern Med. 2007;167(19): 2030. - PubMed
-
- Franzese CB, Stringer SP. The evolution of surgical training: perspectives on educational models from the past to the future. Otolaryngol Clin North Am. 2007;40(6):1227–35. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
