

Cardiac magnetic resonance markers of pre-clinical hypertrophic and dilated cardiomyopathy in genetic variant carriers
- PMID: 40660250
- PMCID: PMC12261545
- DOI: 10.1186/s12916-025-04226-4
Cardiac magnetic resonance markers of pre-clinical hypertrophic and dilated cardiomyopathy in genetic variant carriers
Abstract
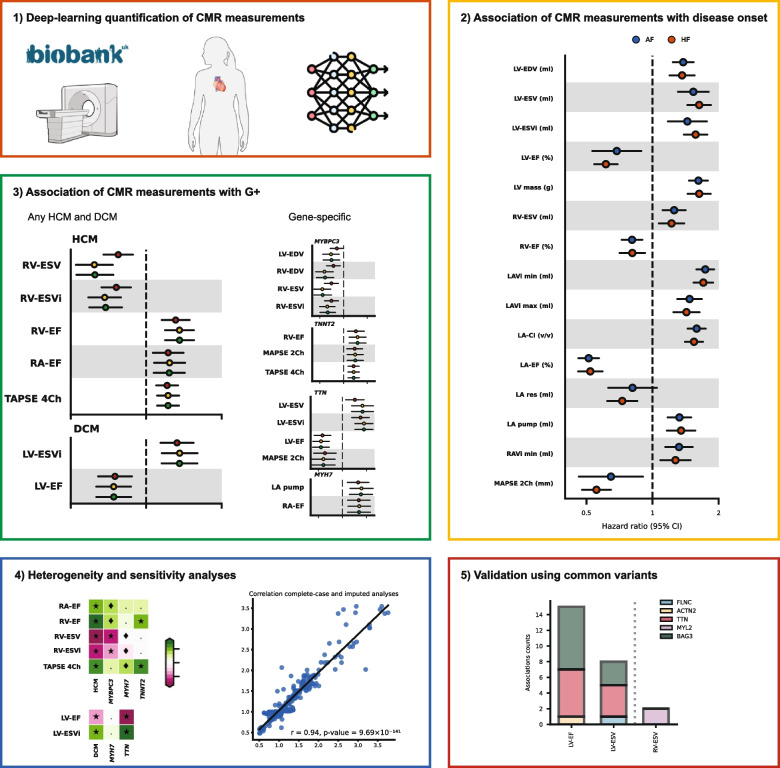
Background: Patients with hypertrophic cardiomyopathy (HCM) and dilated cardiomyopathy (DCM) exhibit structural and functional cardiac abnormalities. We aimed to identify imaging biomarkers for pre-clinical cardiomyopathy in healthy participants carrying cardiomyopathy-associated variants (G +).
Methods: We included 40,169 UK Biobank participants free of cardiac disease at the time of cardiac magnetic resonance imaging (CMR) and with whole exome sequencing. We validated 22 CMR measurements by associating them with incident atrial fibrillation (AF) or heart failure (HF). We subsequently assessed associations of these CMR measurements with HCM G+, DCM G + , or specific genes, utilising generalised linear models conditional on cardiac risk factors.
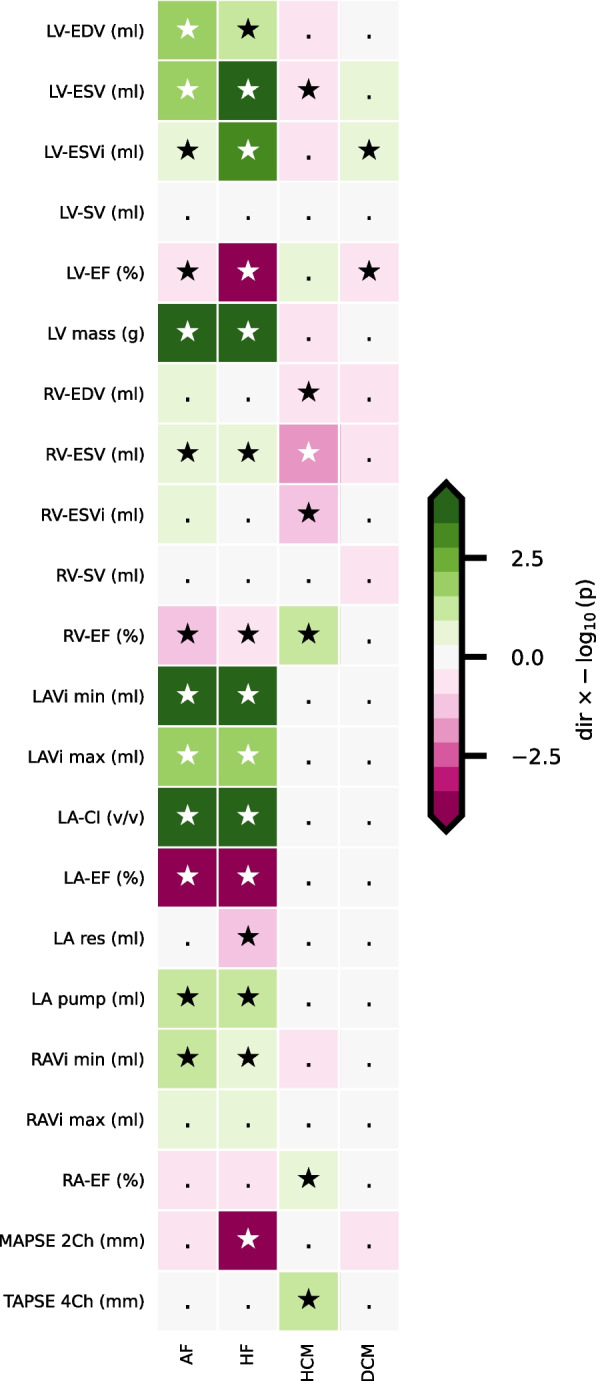
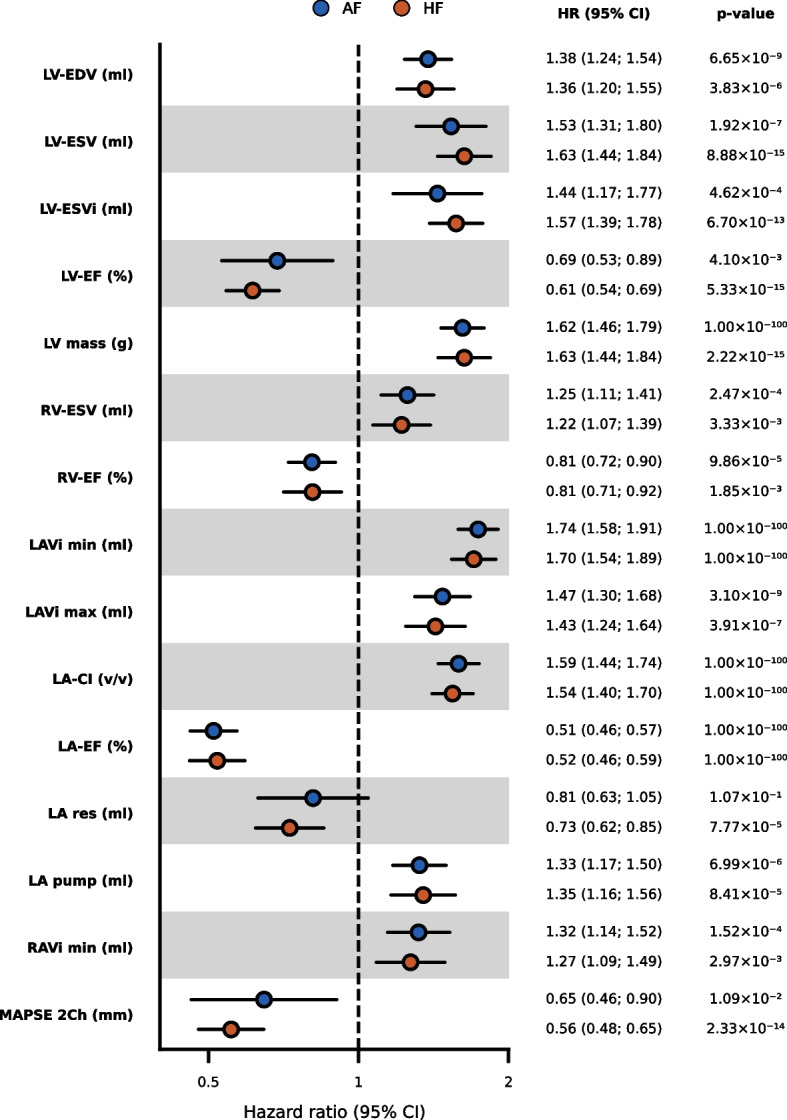
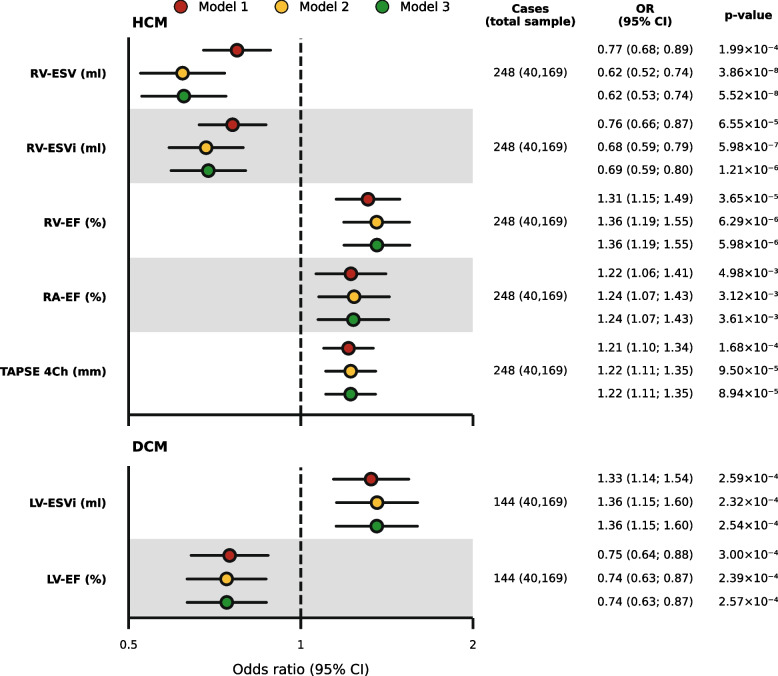
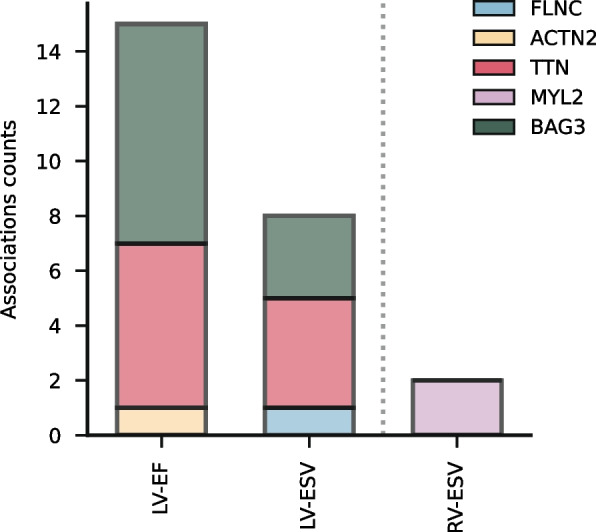
Results: Thirteen CMR measurements were associated with incident AF and 15 with HF. These included left ventricular (LV) ejection fraction (EF; hazard ratio [HR] 0.61, 95% confidence interval [95%CI] 0.54; 0.69) for HF and indexed maximum left atrial volume (LAVi max; HR 1.47, 95%CI 1.29; 1.67) for AF. Five measurements associated with HCM G + , amongst which right ventricular (RV) end-systolic volume (RV-ESV; odds ratio [OR] 0.62, 95%CI 0.53; 0.74), RV-EF (OR 1.36, 95%CI 1.19; 1.55), and right atrial (RA) EF (OR 1.22, 95%CI 1.08; 1.39). Associations overlapping with incident disease and HCM G + had opposite effect directions, such as RV-ESV with HF (HR 1.22, 95%CI 1.07; 1.40). Two CMR measurements associated with DCM G + : LV-ESVi (OR 1.35, 95%CI 1.15; 1.58) and LV-EF (OR 0.75, 95%CI 0.64; 0.88). We observed significant associations with individual cardiomyopathy genes, finding that mitral annular plane systolic excursion associated with TTN and TNNT2, and LA pump volume and RA-EF associated with MYH7.
Conclusions: We identified right-heart CMR measurements associated with HCM G + in healthy individuals, indicating early compensation of cardiac function. LV measurements associated with DCM G + , where CMR associations varied across individual DCM genes, suggesting distinct early pathophysiology.
Keywords: Cardiac magnetic resonance; Dilated cardiomyopathy; Genetics; Hypertrophic cardiomyopathy; Whole exome sequencing.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethics approval for the UKB study was obtained from the North West Centre for Research Ethics Committee (11/NW/0382) and all participants provided informed consent. Consent for publication: Consent for publication is not required, because no details on individuals are reported within the manuscript. Competing interests: AFS has received funding from New Amsterdam Pharma for unrelated projects. PMC is founder, CEO and shareholder of DGTL Health B.V. FWA is supported by UCL Hospitals NIHR Biomedical Research Centre. RK is an Associate Editor of JAMA. He receives support from the National Heart, Lung, and Blood Institute of the National Institutes of Health (under awards R01HL167858 and K23HL153775), the Doris Duke Charitable Foundation (under award 2022060), and the Blavatnik Family Foundation. He also receives research support, through Yale, from Bristol-Myers Squibb, Novo Nordisk, and BridgeBio. He is a coinventor of U.S. Pending Patent Applications 63/562,335, 63/177,117, 63/428,569, 63/346,610, 63/484,426, 63/508,315, and 63/606,203. He is a co-founder of Ensight-AI, Inc. and Evidence2Health, health platforms to improve cardiovascular diagnosis and evidence-based cardiovascular care.
Figures
Update of
-
Cardiac magnetic resonance markers of pre-clinical hypertrophic and dilated cardiomyopathy in genetic variant carriers.medRxiv [Preprint]. 2024 Nov 18:2024.11.15.24317368. doi: 10.1101/2024.11.15.24317368. medRxiv. 2024. Update in: BMC Med. 2025 Jul 15;23(1):421. doi: 10.1186/s12916-025-04226-4. PMID: 39606349 Free PMC article. Updated. Preprint.
References
-
- Arbelo E, Protonotarios A, Gimeno JR, Arbustini E, Barriales-Villa R, Basso C, Bezzina CR, Biagini E, Blom NA, de Boer RA, et al. 2023 ESC guidelines for the management of cardiomyopathies: developed by the task force on the management of cardiomyopathies of the European Society of Cardiology (ESC). Eur Heart J. 2023;44. Available from: https://academic.oup.com/eurheartj/article-abstract/44/37/3503/7246608.
-
- Ingles J, Burns C, Bagnall RD, Lam L, Yeates L, Sarina T, Puranik R, Briffa T, Atherton JJ, Driscoll T, et al. Nonfamilial hypertrophic cardiomyopathy: prevalence, natural history, and clinical implications. Circ Cardiovasc Genet. 2017;10: e001620. - PubMed
-
- Hershberger RE, Hedges DJ, Morales A. Dilated cardiomyopathy: the complexity of a diverse genetic architecture. Nat Rev Cardiol. 2013;10:531–47. - PubMed
-
- Grünig E, Tasman JA, Kücherer H, Franz W, Kübler W, Katus HA. Frequency and phenotypes of familial dilated cardiomyopathy. J Am Coll Cardiol. 1998;31:186–94. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
