

Feasibility of a co-designed and personalised intervention to improve vegetable intake in rural-dwelling young adults
- PMID: 40660295
- PMCID: PMC12257653
- DOI: 10.1186/s12966-025-01796-7
Feasibility of a co-designed and personalised intervention to improve vegetable intake in rural-dwelling young adults
Abstract
Background: This study determined the feasibility, acceptability, engagement and efficacy of a co-designed and personalised digital intervention to increase vegetable intake (Veg4Me) in young (18-to-35 years) rural-dwelling Australian adults.
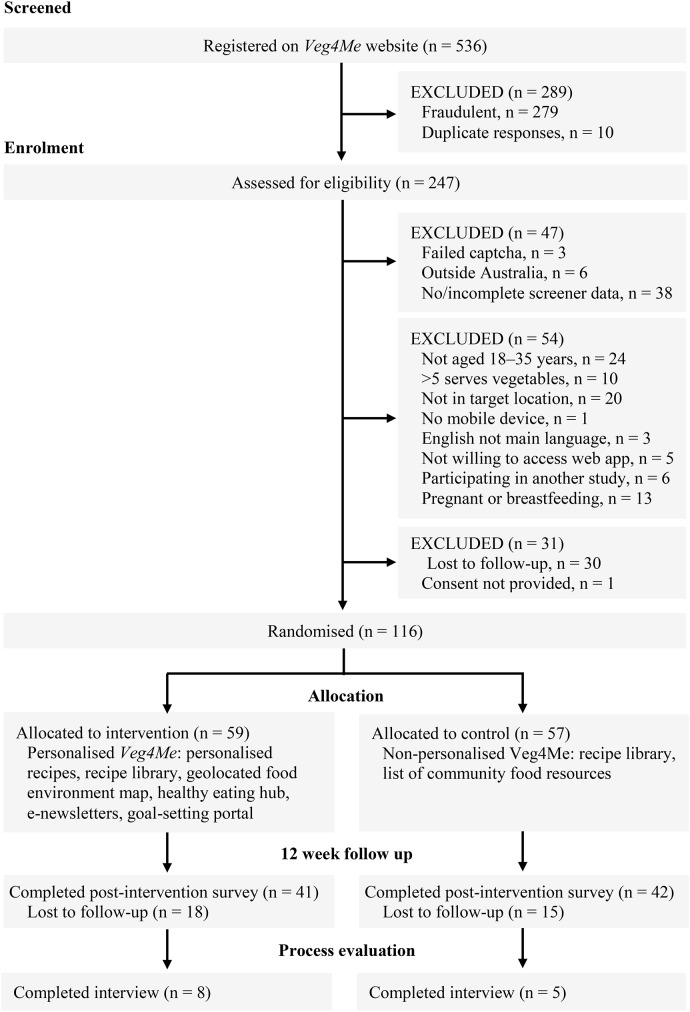
Methods: Participants living in rural Australia were recruited via local government networks and social media and randomised to receive 12-weeks’ access to personalised (intervention) or non-personalised (control) versions of the free Veg4Me web application. The intervention included: (1) personalised recipes, (2) geo-located food environment map, (3) healthy eating resources, (4) goal-setting portal, and (5) personalised e-newsletters. The primary outcome was feasibility (recruitment, participation, and retention rate). Secondary outcomes were user engagement, acceptability, and changes in dietary intake and habits. Descriptive statistics were presented for the intervention and control groups. Generalised linear models estimated group differences in outcomes at 12-weeks.
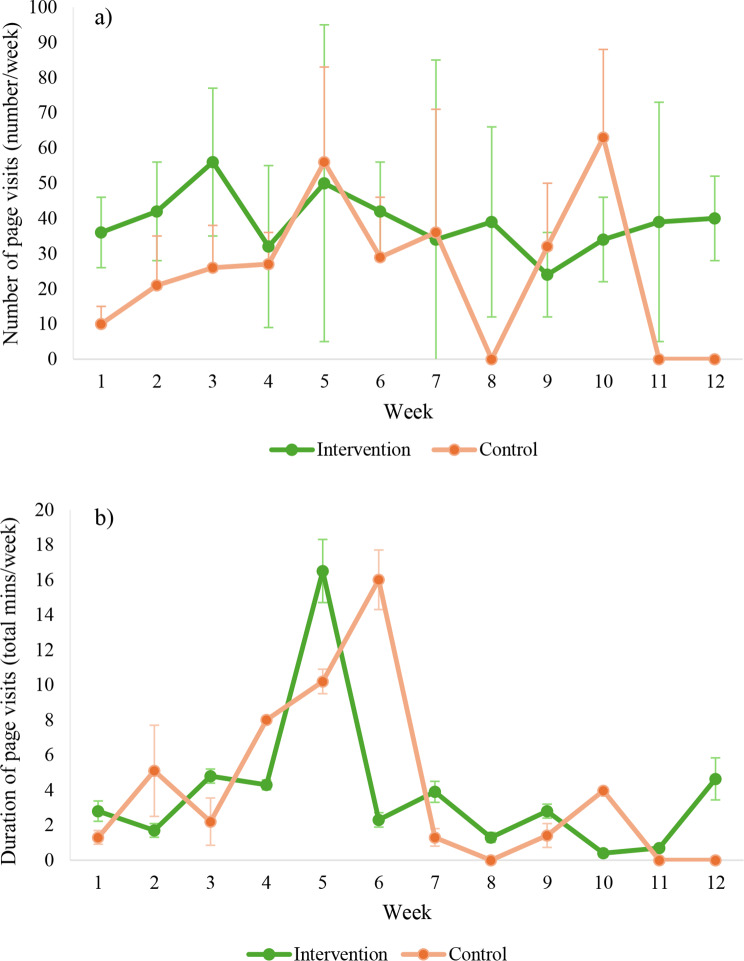
Results: Of the 125 eligible individuals who registered Veg4Me accounts, 116 were randomised and 83 completed postintervention data collection. Recruitment, participation and retention rates were 47%, 93% and 72%, respectively. Intervention participants had higher engagement (median 20 [IQR 3, 54] vs. 6 [IQR 1, 28] page visits/week) and acceptability of the intervention (76%; vs. 52%) than control. Almost all intervention participants liked having access to the recipe library (93%) and reported that the e-newsletters prompted them to access the intervention (90%). Most accessed the goal-setting function (78%), food environment map (76%), and healthy eating resources (63%). More intervention participants reported their vegetable intake had changed in the last 12 weeks, compared with the control (85% vs. 57%; p = 0.010). Mean vegetable intake at 12 weeks for intervention and control was 2.73 (SD 1.1) and 2.66 (SD 1.4) serves/day, respectively (p = 0.76). At 12 weeks, for the intervention and control, confidence to shop regularly for nutritious foods was 68% and 55% (p = 0.09), to cook root vegetables was 88% and 81% (p = 0.11), and to cook pulses was 54% and 48%, respectively (p = 0.52).
Conclusions: A co-designed and personalised digital intervention to increase vegetable intake was feasible, engaging and acceptable among rural-dwelling young adults. Although change in reported vegetable intake was small, findings showed promise for improving dietary intake and habits. Larger trials of effectiveness are needed to determine whether personalised digital interventions can help address health inequities experienced by rural-dwelling young adults.
Trial registration: Australia New Zealand Clinical Trials Registry, ACTRN12623000179639, prospectively registered on 21/02/2023, according to the World Health Organizational Trial Registration Data Set. Universal Trial Number U1111-1284-9027.
Supplementary Information: The online version contains supplementary material available at 10.1186/s12966-025-01796-7.
Keywords: Diet; Intervention; Rural; Vegetable intake; Young adults.
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by Deakin University’s Human Ethics Advisory Group– Health (HEAG-H 06_2023). Written informed consent was obtained from all participants. The datasets generated and/or analyses generated will not be publicly available but may be made available by the first author on reasonable request and upon approval by the Deakin Human Ethics Advisory Group Consent for publication: Not applicable. Competing interests: KML is an Associate Editor for the International Journal of Behavioral Nutrition and Physical Activity. KML was not involved in the journal’s peer review process of, or decisions related to, this manuscript. All other authors declare that they have no competing interests.
Figures


Similar articles
-
Efficacy and External Validity of Electronic and Mobile Phone-Based Interventions Promoting Vegetable Intake in Young Adults: Systematic Review and Meta-Analysis.J Med Internet Res. 2016 Apr 8;18(4):e58. doi: 10.2196/jmir.5082. J Med Internet Res. 2016. PMID: 27059765 Free PMC article.
-
Co-design of a personalised digital intervention to improve vegetable intake in adults living in Australian rural communities.BMC Public Health. 2024 Jan 10;24(1):146. doi: 10.1186/s12889-024-17641-8. BMC Public Health. 2024. PMID: 38200514 Free PMC article.
-
Evaluating a 52-week fresh food prescribing program in Ontario, Canada: A mixed-methods study on food insecurity, fruit and vegetable intake, and health.BMC Prim Care. 2025 Jul 2;26(1):208. doi: 10.1186/s12875-025-02907-w. BMC Prim Care. 2025. PMID: 40604564 Free PMC article.
-
Interventions for increasing fruit and vegetable consumption in children aged five years and under.Cochrane Database Syst Rev. 2024 Sep 23;9(9):CD008552. doi: 10.1002/14651858.CD008552.pub8. Cochrane Database Syst Rev. 2024. PMID: 39312396
-
Determining the feasibility of a codesigned and personalised intervention (Veg4Me) to improve vegetable intake in young adults living in rural Australian communities: protocol for a randomised controlled trial.BMJ Open. 2024 Jan 11;14(1):e078001. doi: 10.1136/bmjopen-2023-078001. BMJ Open. 2024. PMID: 38216197 Free PMC article.
References
-
- Australian Institute of Health Welfare. Rural and remote health 2019 [Available from: https://www.aihw.gov.au/reports/rural-remote-australians/rural-remote-he...]
-
- Alston L, Allender S, Peterson K, Jacobs J, Nichols M. Rural inequalities in the Australian burden of ischaemic heart disease: A systematic review. Heart Lung Circ. 2017;26(2):122–33. - PubMed
-
- Chisholm M, Russell D, Humphreys J. Measuring rural allied health workforce turnover and retention: what are the patterns, determinants and costs? Aust J Rural Health. 2011;19(2):81–8. - PubMed
-
- OECD. Delivering Quality Education and Health Care to All2021.
-
- Australian Bureau of Statistics. National Health Survey. 2017-18: First results 2018 [Available from: https://www.abs.gov.au/statistics/health/health-conditions-and-risks/nat...]
Grants and funding
LinkOut - more resources
Full Text Sources
