

Kinesin-related genes stratified the prognosis and immune responses of clear cell renal cell carcinoma
- PMID: 40660314
- PMCID: PMC12261704
- DOI: 10.1186/s40001-025-02880-1
Kinesin-related genes stratified the prognosis and immune responses of clear cell renal cell carcinoma
Abstract
Background: Clear cell renal cell carcinoma (ccRCC) is a prevalent and aggressive form of kidney cancer. Recently, the identification of suitable subtypes in ccRCC for the prediction of prognosis and immune infiltration remains limited. Kinesin superfamily proteins (KIFs), a group of molecular motor proteins, have been found to play crucial roles in tumor progression and patient prognosis in various cancers. However, the subtypes in ccRCC based on KIFs remain poorly understood.
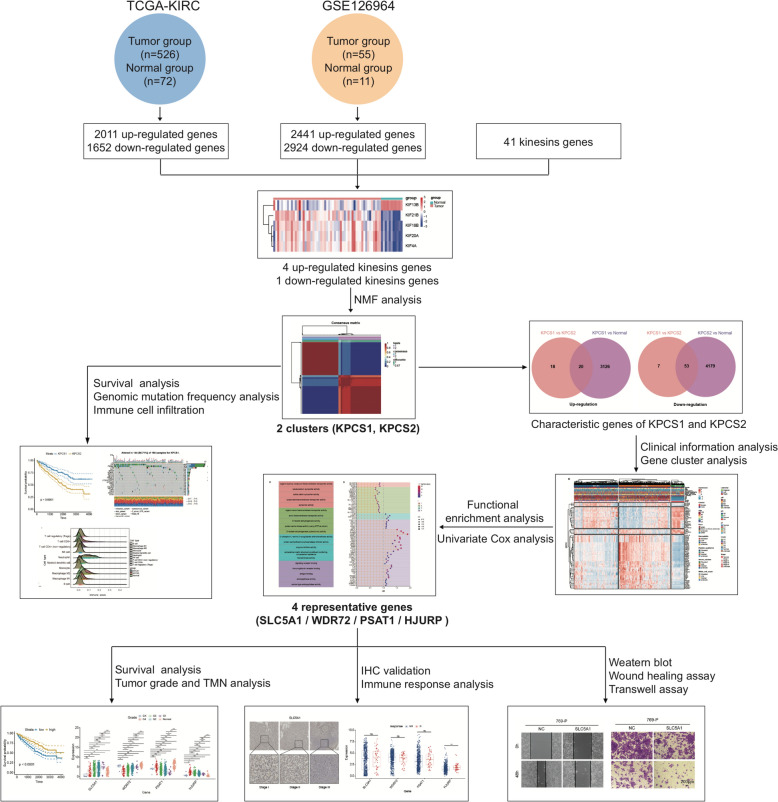
Methods: In this study, transcriptional profiles of ccRCC were analyzed using data from the Gene Expression Omnibus (GEO) and The Cancer Genome Atlas (TCGA) databases. Differential expression of KIFs was identified using R software. Subsequently, ccRCC patients were stratified into two distinct subgroups based on non-negative matrix factorization (NMF) analysis. Comparative analyses were performed to evaluate prognosis, mutations, and immune cell infiltration between these subtypes. Furthermore, signature genes associated with the identified subtypes were determined, followed by an investigation into their relationship with clinical characteristics and response to immune checkpoint inhibitors. Validation studies involving immunohistochemical staining, malignant phenotype assays, and immunofluorescence were conducted to assess the expression and function of these signature genes.
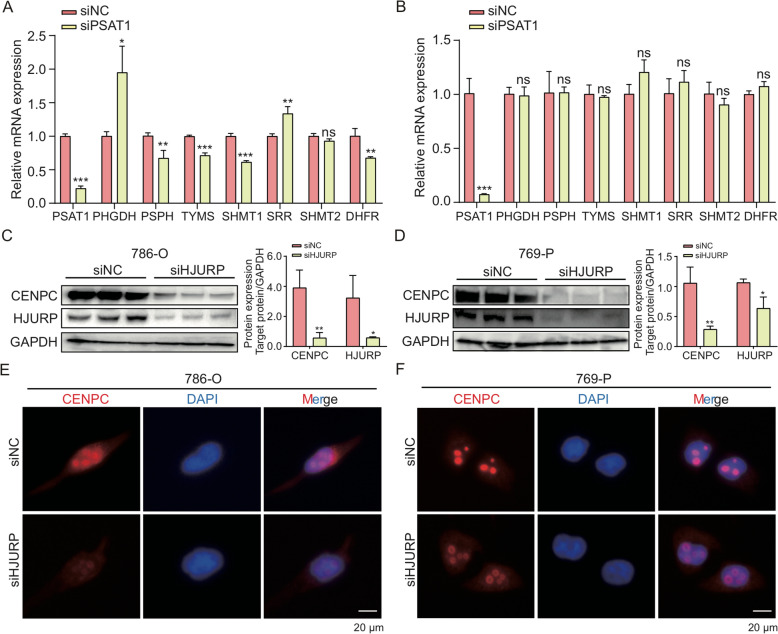
Results: Five KIFs genes, namely, KIF21B, KIF18B, KIF20A, KIF4A, and KIF13B, were identified as classifiers for categorizing ccRCC patients into two distinct subtypes known as KPCS1 and KPCS2. The aggressive subtype, KPCS2, was found to be associated with poorer survival outcomes. Furthermore, higher immune infiltration and copy number variations were observed in the KPCS2 subtype. Four signature genes (SLCA15, WDR72, PSAT1, and HJURP) displayed significant correlations with clinical characteristics and were determined to be linked to the ccRCC subtypes. The expression patterns and functional roles of these signature genes were subsequently validated in both ccRCC cells and tissues.
Conclusion: KIFs-associated subtypes provide valuable insights into the molecular characteristics and prognostic implications of ccRCC, thereby suggesting potential therapeutic targets for intervention.
Keywords: Clear cell renal cell carcinoma; Immune response; Kinesin superfamily proteins; Molecular subtypes; Targets.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The human tissue samples in this study were approved by the Institutional Review Board of the Shanghai Outdo Biotech Company (Approved number: SHYJS-CP-1501008; Approved date: Jan 02nd, 2015). Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures






Similar articles
-
A prognostic microRNA-based signature for localized clear cell renal cell carcinoma: the Bio-miR study.Br J Cancer. 2025 Aug;133(2):155-167. doi: 10.1038/s41416-025-03008-2. Epub 2025 May 7. Br J Cancer. 2025. PMID: 40335662
-
Multi-omics analysis of zinc finger protein 683 as a prognostic biomarker for immune infiltration in clear cell renal cell carcinoma.BMC Cancer. 2025 Jul 29;25(1):1236. doi: 10.1186/s12885-025-14643-6. BMC Cancer. 2025. PMID: 40730958 Free PMC article.
-
Machine Learning-Based Pathomics Model to Predict the Prognosis in Clear Cell Renal Cell Carcinoma.Technol Cancer Res Treat. 2024 Jan-Dec;23:15330338241307686. doi: 10.1177/15330338241307686. Technol Cancer Res Treat. 2024. PMID: 39703069 Free PMC article.
-
A Systematic Review and Meta-analysis Comparing the Effectiveness and Adverse Effects of Different Systemic Treatments for Non-clear Cell Renal Cell Carcinoma.Eur Urol. 2017 Mar;71(3):426-436. doi: 10.1016/j.eururo.2016.11.020. Epub 2016 Dec 8. Eur Urol. 2017. PMID: 27939075
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.Health Technol Assess. 2006 Sep;10(34):iii-iv, ix-xi, 1-204. doi: 10.3310/hta10340. Health Technol Assess. 2006. PMID: 16959170
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global cancer statistics 2020: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49. - PubMed
-
- Petejova N, Martinek A. Renal cell carcinoma: review of etiology, pathophysiology and risk factors. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2016;160(2):183–94. - PubMed
-
- Ahrens M, Scheich S, Hartmann A, Bergmann L. Society I-NIWGKCotGC: non-clear cell renal cell carcinoma—pathology and treatment options. Oncol Res Treat. 2019;42(3):128–35. - PubMed
-
- Lara PN Jr, Evans CP. Cytoreductive nephrectomy in metastatic renal cell cancer: not all that it’s cut out to be. JAMA Oncol. 2019;5(2):171–2. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
