

Validation of the Delirium Diagnostic Tool-Provisional in intensive care units
- PMID: 40660596
- PMCID: PMC12263007
- DOI: 10.1097/MD.0000000000043212
Validation of the Delirium Diagnostic Tool-Provisional in intensive care units
Abstract
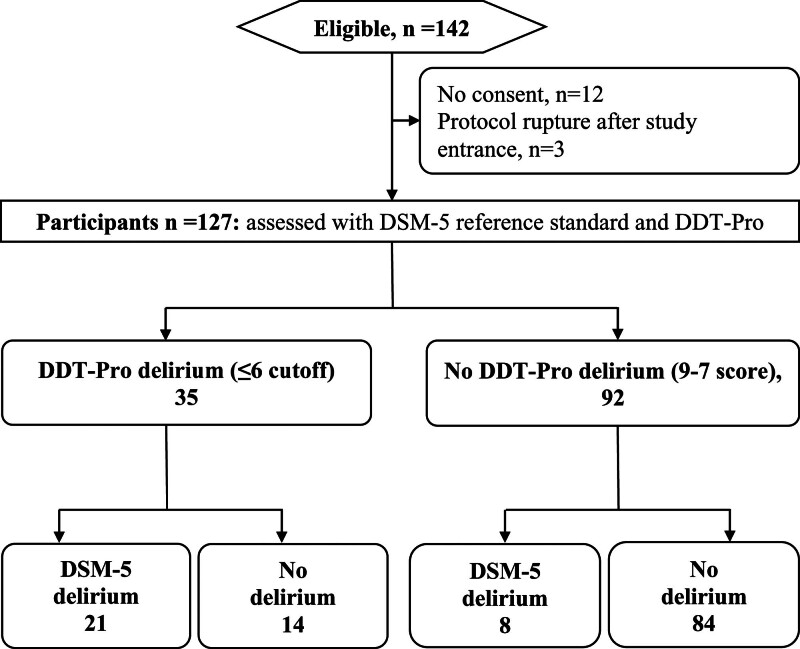
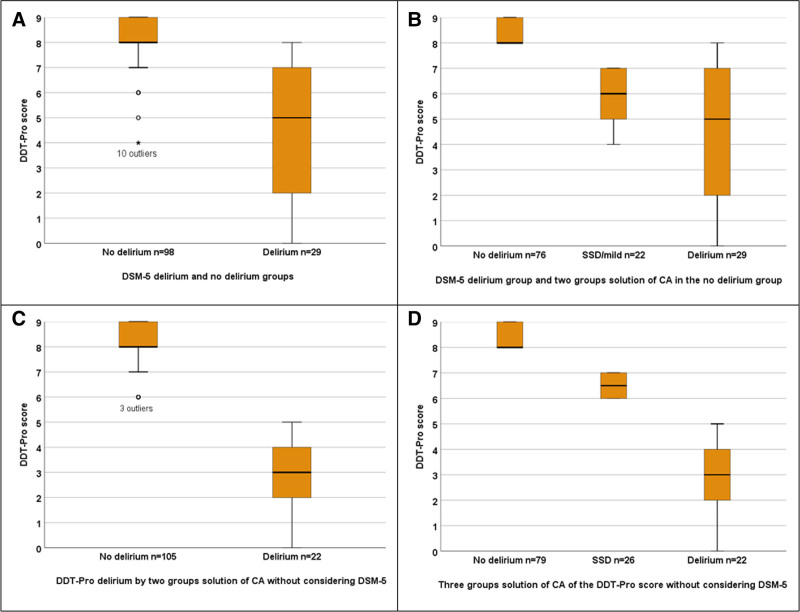
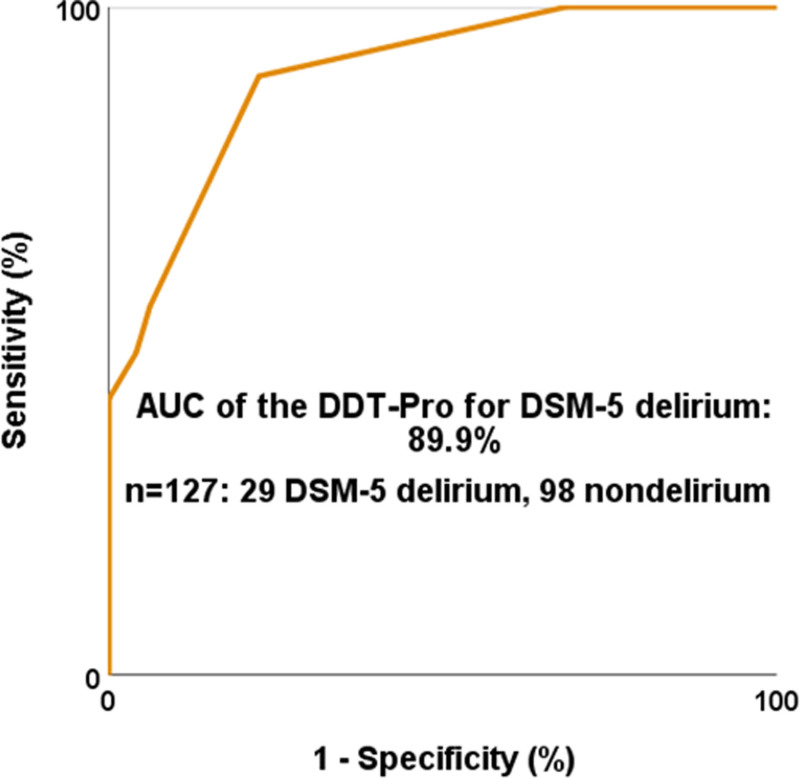
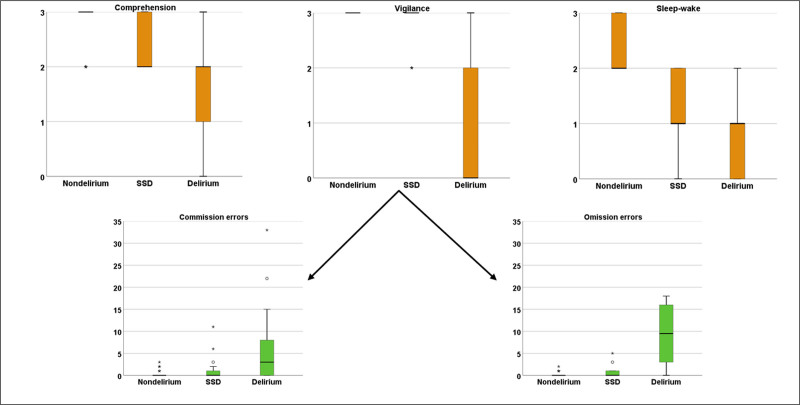
Shortcomings of intensive care units (ICU) delirium screening tools include not measuring its core features, not excluding stupor/coma and not being continuous measurement instruments. We validated the Delirium Diagnostic Tool-Provisional (DDT-Pro) that assesses all 3 core symptom domains for delirium and subsyndromal delirium (SSD) in the ICU. This is a multicenter validation following STARD guideline. Delirium reference standards were DSM-5 criteria, cluster analysis (CA) of the DDT-Pro scores and clinical validators for preestablished DDT-Pro ≤ 6 and ≤ 7 cutoffs (0-9 range) for delirium and SSD. DDT-Pro dimensionality and internal consistency reliability are reported. Of 127 patients, 29 (22.8%) had DSM-5 delirium. The area under the receiver-operator DDT-Pro curve was 90% with the ≤ 7 and ≤ 6 DDT-Pro cutoffs which had 82.7% and 80.3% accuracy at the most balanced sensitivity-specificity. The ≤ 6 cutoff specificity (85.7%) was higher, while ≤ 7 cutoff sensitivity (89.7%) was higher with NPV = 96.2%. According to CA, ≤7 cutoff differentiated 100% of nondelirium patients from SSD and delirium, whereas DSM-5 misattributed SSD. Validation of an SSD group was supported by delirium severity gradients and various clinical validators. Cases in this CA also coincided exactly with nondelirium, SSD and delirium groups prespecified by DDT-Pro cutoffs from non-ICU samples. One factor explained 69.9% of the DDT-Pro variance, Cronbach α = 0.79 (cohesive delirium dimension). Our findings indicate that the DDT-Pro has very good construct validity and discriminates ICU delirium against DSM-5, performing even more cleanly using agnostic CA for SSD and delirium diagnosis. Its continuous score structure discernment of SSD was supported by clinical validators. ICU cutoffs were the same as in previous inpatient samples.
Keywords: cluster analysis; delirium screening; intensive care unit; sensitivity and specificity.
Copyright © 2025 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
Dr. P. Trzepacz holds the copyright for the Delirium Rating Scale-Revised-98 (she does not charge a fee for not-for-profit use of this instrument), and she receives a pension from and is a shareholder with Eli Lilly. Dr. P. Trzepacz and Dr. J. Franco are co-owners of the copyright for the Delirium Diagnostic Tool-Provisional (they do not charge a fee for not-for-profit use of this instrument). The other authors have no conflicts of interest to disclose.
Figures
References
-
- Rood P, Huisman-de Waal G, Vermeulen H, Schoonhoven L, Pickkers P, van den Boogaard M. Effect of organisational factors on the variation in incidence of delirium in intensive care unit patients: a systematic review and meta-regression analysis. Aust Crit Care. 2018;31:180–7. - PubMed
-
- Trzepacz PT. Update on the neuropathogenesis of delirium. Dement Geriatr Cogn Disord. 1999;10:330–4. - PubMed
-
- Franco JG, Trzepacz PT, Meagher DJ, et al. Three core domains of delirium validated using exploratory and confirmatory factor analyses. Psychosomatics. 2013;54:227–38. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
