

Improving efficiency in lung SAbR planning using integrated tools for X-ray based adaptive radiotherapy
- PMID: 40660864
- PMCID: PMC12260260
- DOI: 10.1002/acm2.70195
Improving efficiency in lung SAbR planning using integrated tools for X-ray based adaptive radiotherapy
Abstract
Purpose: To evaluate the feasibility of translating clinical lung stereotactic ablative radiotherapy (SAbR) templates from Ethos1.1 to Ethos2.0, leveraging new features to facilitate dose fall-off and automate patient-specific beam arrangement. This study aims to streamline planning processes and support broader adoption of online adaptive radiotherapy (ART) for lung SAbR.
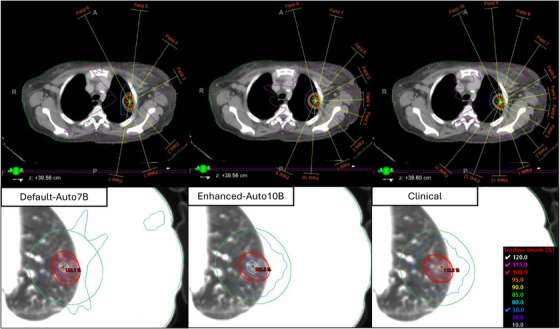
Methods: We selected fifteen patients previously treated with adaptive lung SAbR using the Ethos1.1 system, each receiving 40-60 Gy in 5 fractions. Plans were reoptimized in Ethos2.0 using identical parameters (rIMRT) to their clinical counterpart. To evaluate new integrated features, we utilized high-fidelity (HF) mode with and without automatic treatment geometry selection (HF-cIMRT, HF-aIMRT/VMAT). These strategies were compared to assess the impact of Ethos2.0's new features on plan quality and efficiency using RTOG-based metrics and enhanced plan deliverability analysis. Statistical significance was assessed using paired Student's t-tests (α = 0.05).
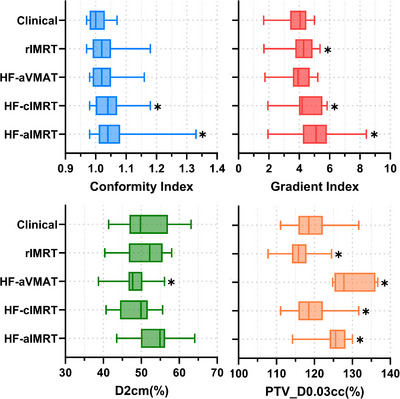
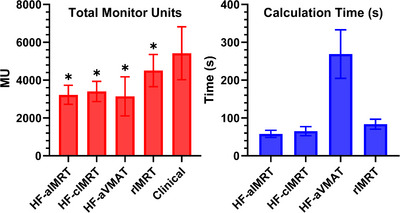
Results: All plans reoptimized in Ethos2.0 demonstrated acceptable plan quality. No statistically significant differences in maximum organ-at-risk doses were observed between evaluated strategies and the clinical plan. For complex cases, human-selected beam geometry proved superior to automated geometry. HF-enabled plans significantly reduced total monitor units, with HF-aVMAT, HF-cIMRT, and HF-aIMRT reporting 3142.4 ± 997.4 (p < 0.001), 3401.8 ± 516.1 (p < 0.001), and 3225.6 ± 484.2 (p < 0.001) compared to clinical 5424.9 ± 1353.4. A trade-off was observed in conformity index, which was 1.06 ± 0.08 (p = 0.006), 1.05 ± 0.06 (p = 0.003), and 1.03 ± 0.05 (p = 0.05) for HF-aIMRT, HF-cIMRT, and HF-aVMAT plans compared to clinical 1.01 ± 0.03.
Conclusion: Lung SAbR planning strategies can be effectively transitioned from Ethos1.1 to Ethos2.0, improving workflow efficiency with high-fidelity mode and minor adjustments. Automated beam geometry tools enhance planner efficiency for both IMRT and VMAT. To address increased ART workload and staffing demands, leveraging integrated automation tools is essential. The planning strategies presented in this study are straightforward and reproducible for ART-enabled clinics.
Keywords: SAbR; adaptive radiotherapy; automation; lung‐SBRT.
© 2025 The Author(s). Journal of Applied Clinical Medical Physics published by Wiley Periodicals, LLC on behalf of The American Association of Physicists in Medicine.
Conflict of interest statement
No conflicts of interest.
Figures
Similar articles
-
Non-coplanar VMAT plans for lung SABR to reduce dose to the heart: a planning study.Br J Radiol. 2020 Jan;93(1105):20190596. doi: 10.1259/bjr.20190596. Epub 2019 Oct 22. Br J Radiol. 2020. PMID: 31625759 Free PMC article.
-
Evaluation of the efficacy of automated machine learning enhanced planning system and a comparative analysis with manual planning system.J Cancer Res Ther. 2025 Apr 1;21(3):593-601. doi: 10.4103/jcrt.jcrt_1373_24. Epub 2025 Jul 5. J Cancer Res Ther. 2025. PMID: 40616541
-
Biological adaptive radiotherapy for short-time dose compensation in lung SBRT patients.Med Phys. 2025 Jul;52(7):e17820. doi: 10.1002/mp.17820. Epub 2025 Apr 14. Med Phys. 2025. PMID: 40229143
-
Stereotactic body radiotherapy for early-stage lung cancer: a systematic review on the choice of photon energy and linac flattened/unflattened beams.Radiat Oncol. 2024 Jan 2;19(1):1. doi: 10.1186/s13014-023-02392-4. Radiat Oncol. 2024. PMID: 38167095 Free PMC article.
-
Palliative radiotherapy regimens for patients with thoracic symptoms from non-small cell lung cancer.Cochrane Database Syst Rev. 2015 Jan 14;1(1):CD002143. doi: 10.1002/14651858.CD002143.pub4. Cochrane Database Syst Rev. 2015. PMID: 25586198 Free PMC article.
References
-
- Archambault Y, Boylan C, Bullock D, et al. Making on‐line adaptive radiotherapy possible using artificial intelligence and machine learning for efficient daily re‐planning. Med Phys Intl J. 2020;8(2).
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
