

Spinal dural arteriovenous fistulas presenting as intracranial subarachnoid hemorrhage: A systematic review
- PMID: 40660916
- PMCID: PMC12264256
- DOI: 10.1177/15910199251328721
Spinal dural arteriovenous fistulas presenting as intracranial subarachnoid hemorrhage: A systematic review
Abstract
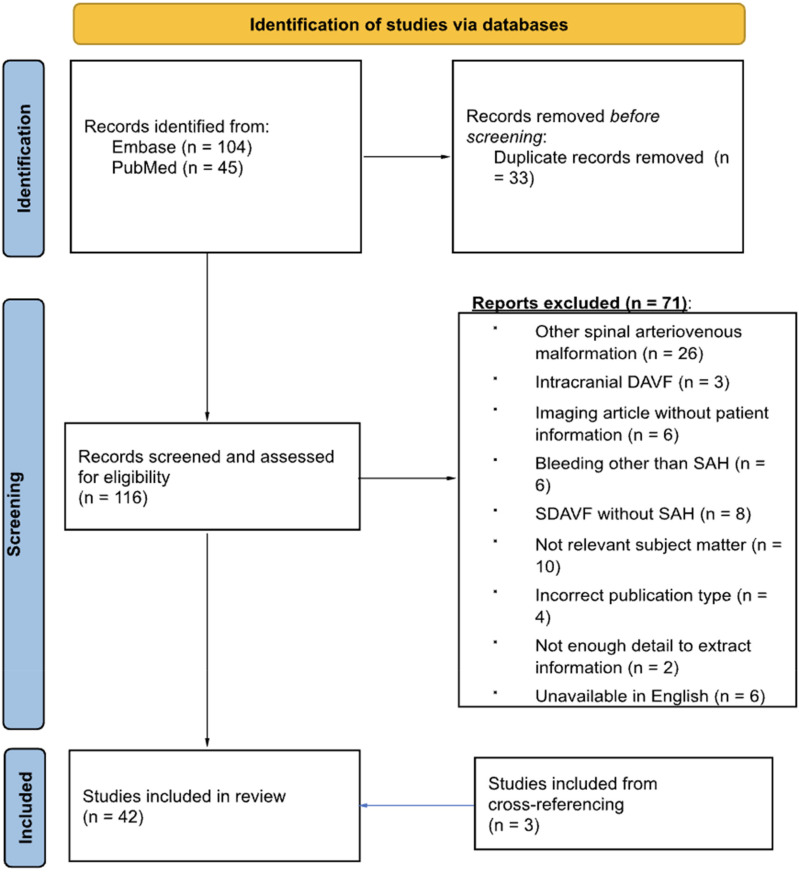
BackgroundSpinal dural arteriovenous fistulas (SDAVFs) are the most common type of spinal arteriovenous malformation. Typically, these malformations present with a wide range of nonspecific symptoms indicative of thoracolumbar myelopathy. However, patients with spinal dural arteriovenous fistulas may rarely present with subarachnoid hemorrhage.MethodsA systematic review of MEDLINE and Embase databases was performed querying for cases of spinal dural arteriovenous fistulas with subarachnoid hemorrhage. Patient characteristics and outcomes investigated included spinal level of the fistula, delay of diagnosis, Hunt and Hess grade, interventions, recurrence of the fistula, and postoperative disability. Additionally, we present a unique case in which subarachnoid hemorrhage resulted from a spinal dural arteriovenous fistula that was refractory to multiple endovascular and open surgical interventions.ResultsOf 116 records identified, 45 studies were included comprising 80 patients with spinal dural arteriovenous fistula and subarachnoid hemorrhage. The most common locations of the spinal dural arteriovenous fistula were in the cervical spine (57.5%) and at the craniocervical junction (35%). Patients were treated with open surgical ligation (60.0%), endovascular embolization (22.5%), or an open surgical procedure following persistent symptoms after endovascular treatment (10.0%). Overall, the prognoses among the treated patients were favorable with only two reported (2.5%) mortalities. Rates of neurologic recovery were similar when comparing endovascular and open surgical treatment. Endovascular treatment with coil embolization of a C1-C2 spinal dural arteriovenous fistula presenting as subarachnoid hemorrhage is also described.ConclusionSpinal dural arteriovenous fistulas, particularly in the cervical spine, could be considered as a potential etiology for subarachnoid hemorrhage patients with no obvious intracranial cause. Treatment with either open surgery or embolization appears to offer a positive prognosis for both functional and angiographic outcomes.
Keywords: Onyx™; Spinal dural arteriovenous fistula; embolization; endovascular; n-butyl cyanoacrylate; subarachnoid hemorrhage.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

Similar articles
-
Multimodality treatment maximizing outcome in spinal dural arteriovenous fistulae.J Clin Neurosci. 2025 Aug 22;141:111571. doi: 10.1016/j.jocn.2025.111571. Online ahead of print. J Clin Neurosci. 2025. PMID: 40848625
-
Endovascular Treatment for Tentorial Dural Arteriovenous Fistulas: A Retrospective Single-Center Study.AJNR Am J Neuroradiol. 2025 Aug 1;46(8):1617-1624. doi: 10.3174/ajnr.A8676. AJNR Am J Neuroradiol. 2025. PMID: 39880688
-
Feasibility, safety, and efficacy of endovascular treatment of anterior cranial fossa dural arteriovenous fistulas: a systematic review and meta-analysis with a subanalysis for Onyx.Neurosurg Rev. 2024 May 13;47(1):217. doi: 10.1007/s10143-024-02446-5. Neurosurg Rev. 2024. PMID: 38736006
-
Characteristics and outcomes of pediatric dural arteriovenous fistulas: a systematic review.Childs Nerv Syst. 2024 Jan;40(1):197-204. doi: 10.1007/s00381-023-06156-z. Epub 2023 Oct 21. Childs Nerv Syst. 2024. PMID: 37864710
-
Dural arteriovenous fistulas at the craniocervical junction: a systematic review.J Neurointerv Surg. 2016 Jun;8(6):648-53. doi: 10.1136/neurintsurg-2015-011775. Epub 2015 Jun 3. J Neurointerv Surg. 2016. PMID: 26041099
References
-
- Fassett DR, Rammos SK, Patel P, et al. Intracranial subarachnoid hemorrhage resulting from cervical spine dural arteriovenous fistulas: literature review and case presentation. Neurosurg Focus 2009; 26: E4. - PubMed
-
- Marcus J, Schwarz J, Singh IP, et al. Spinal dural arteriovenous fistulas: a review. Curr Atheroscler Rep 2013; 15: 335. - PubMed
-
- Yue H, Ling W, Ou Y, et al. Intracranial subarachnoid hemorrhage resulting from non-cervical spinal arteriovenous lesions: analysis of possible cause of bleeding and literature review. Clin Neurol Neurosurg 2019; 184: 105371. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
